

The caretaker-reversible Tarsorrhaphy
- PMID: 39352581
- PMCID: PMC11445321
- DOI: 10.1007/s10792-024-03310-7
The caretaker-reversible Tarsorrhaphy
Abstract
Purpose: To present a modification of the reversible tarsorrhaphy that can be opened and reclosed as necessary by caretakers and the patient.
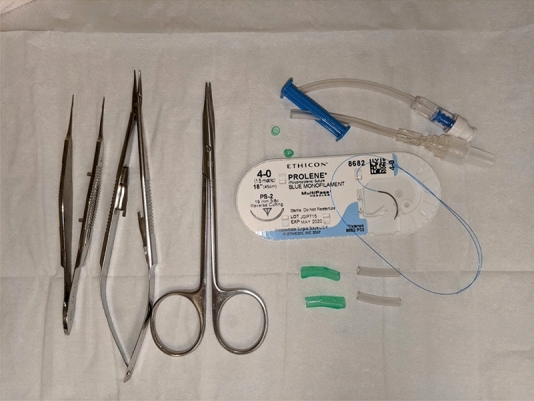
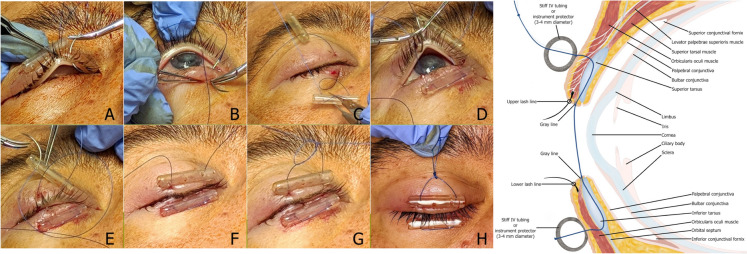
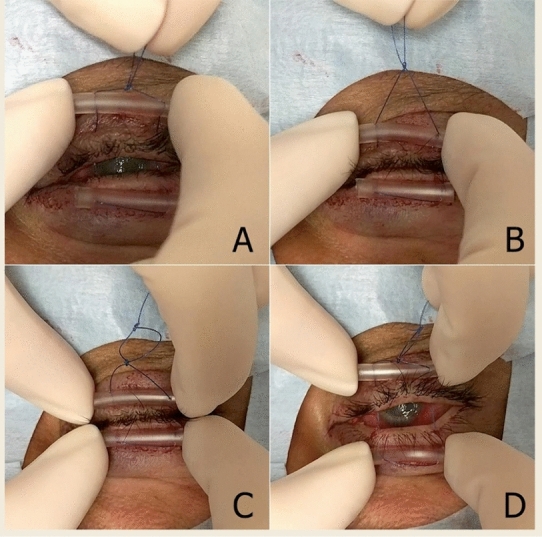
Methods: Retrospective case series of patients who underwent the reversible tarsorrhaphy. Materials included intravenous (IV) tubing as bolsters and 4-0 polypropylene suture. The 4-0 suture is first passed through and through one end of IV tubing approximately 20 mm in length. Starting on the lateral upper lid and approximately 4 mm above the lash line, the suture is placed through the skin and into the tarsus. The suture exits through the eyelid gray line. These steps through the eyelid are repeated in the opposite direction. An air knot is tied above the upper eyelid near the base of IV tubing. A second air knot can be tied higher to provide a handle easily allowing the caretaker to close the eyelid.
Results: Included were 13 patients (ages 21-95-yeas), indications included lagophthalmos secondary to cicatricial changes from burns (2), keratouveitis (1), neurogenic palsy (3), neurotrophic ulcer (6), and cicatricial changes from skin cancer (1). There were no reported difficulties in maintaining the tarsorrhaphy by either family members or healthcare providers. The first tarsorrhaphy for each patient lasted between 3-19 weeks, with an average of 8 weeks. All were well tolerated.
Conclusions: The caretaker-reversible tarsorrhaphy can be used as a temporizing measure. The technique balances the need for ocular protection with the need for examination/treatment by health care professionals and, equally importantly, the patients and caretakers.
Keywords: Cornea; Oculoplastic surgery; Oculoplastics; Tarsorrhaphy.
© 2024. The Author(s).
Conflict of interest statement
The authors have not disclosed any competing interests.
Figures
References
-
- Grob S, Charlson E, Tao J (2020) Tarsorrhaphy (Temporary and Permanent). In: ophthalmic plastic surgery: tricks of the trade. Georg Thieme Verlag b-006-163725 10.1055/b-006-163725
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
