

Type 2 diabetes mellitus in adults: pathogenesis, prevention and therapy
- PMID: 39353925
- PMCID: PMC11445387
- DOI: 10.1038/s41392-024-01951-9
Type 2 diabetes mellitus in adults: pathogenesis, prevention and therapy
Abstract
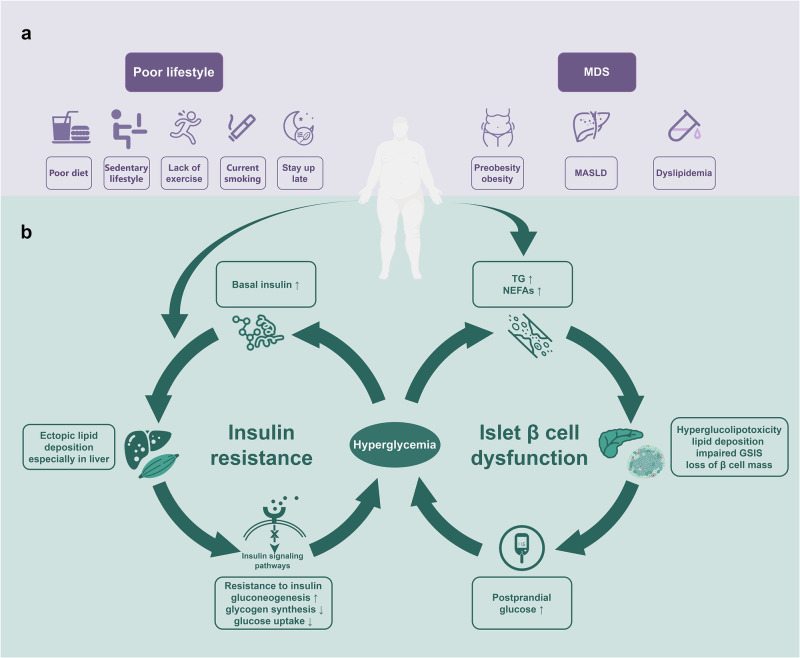
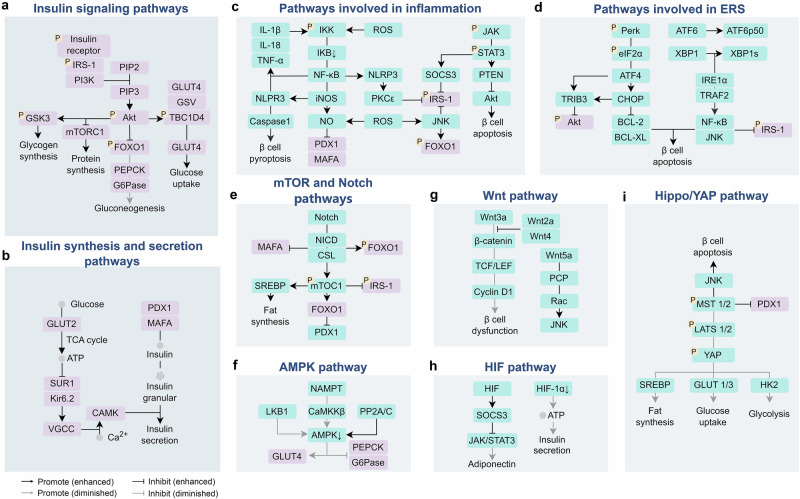
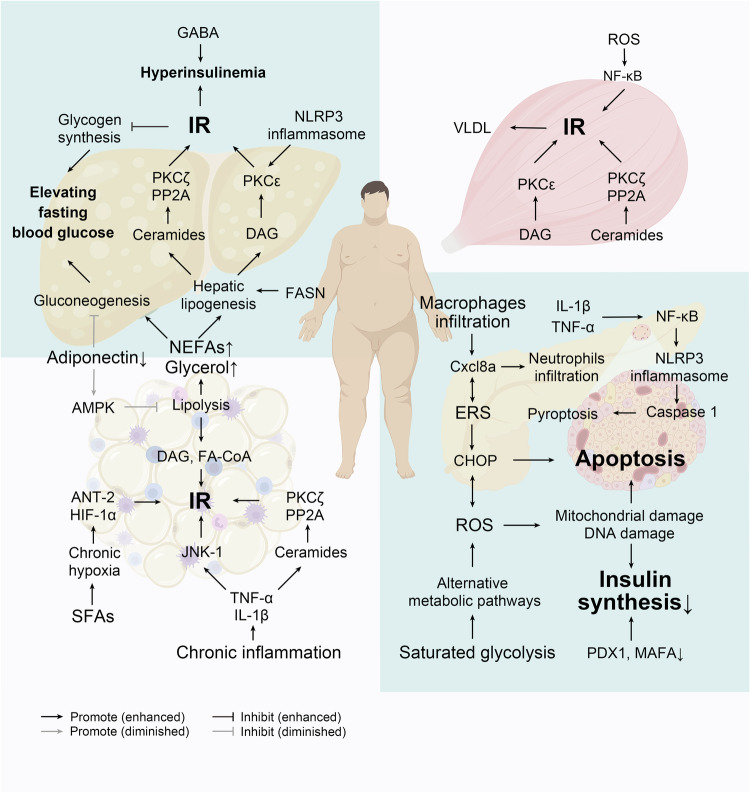
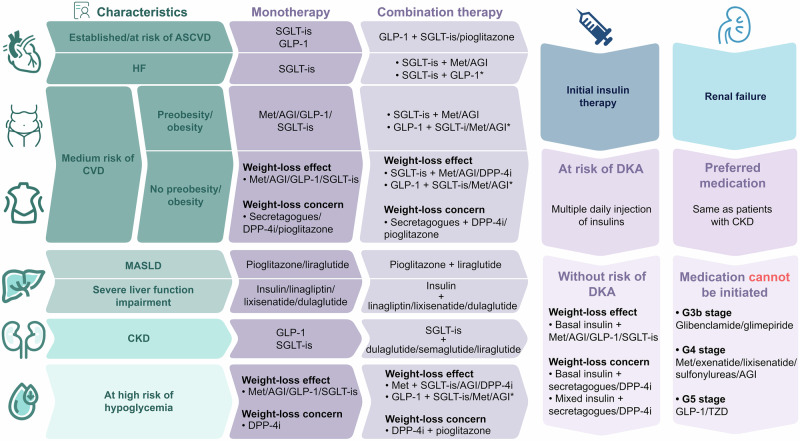
Type 2 diabetes (T2D) is a disease characterized by heterogeneously progressive loss of islet β cell insulin secretion usually occurring after the presence of insulin resistance (IR) and it is one component of metabolic syndrome (MS), and we named it metabolic dysfunction syndrome (MDS). The pathogenesis of T2D is not fully understood, with IR and β cell dysfunction playing central roles in its pathophysiology. Dyslipidemia, hyperglycemia, along with other metabolic disorders, results in IR and/or islet β cell dysfunction via some shared pathways, such as inflammation, endoplasmic reticulum stress (ERS), oxidative stress, and ectopic lipid deposition. There is currently no cure for T2D, but it can be prevented or in remission by lifestyle intervention and/or some medication. If prevention fails, holistic and personalized management should be taken as soon as possible through timely detection and diagnosis, considering target organ protection, comorbidities, treatment goals, and other factors in reality. T2D is often accompanied by other components of MDS, such as preobesity/obesity, metabolic dysfunction associated steatotic liver disease, dyslipidemia, which usually occurs before it, and they are considered as the upstream diseases of T2D. It is more appropriate to call "diabetic complications" as "MDS-related target organ damage (TOD)", since their development involves not only hyperglycemia but also other metabolic disorders of MDS, promoting an up-to-date management philosophy. In this review, we aim to summarize the underlying mechanism, screening, diagnosis, prevention, and treatment of T2D, especially regarding the personalized selection of hypoglycemic agents and holistic management based on the concept of "MDS-related TOD".
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes-2024. Diabetes Care47 (2024).
Publication types
MeSH terms
Grants and funding
- 82170830/National Natural Science Foundation of China (National Science Foundation of China)
- 82170830/National Natural Science Foundation of China (National Science Foundation of China)
- 82170830/National Natural Science Foundation of China (National Science Foundation of China)
- 82170830/National Natural Science Foundation of China (National Science Foundation of China)
- 82170830/National Natural Science Foundation of China (National Science Foundation of China)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
