

Normal Variants and Pitfalls of 18F-FDG PET/CT Imaging in Pediatric Oncology
- PMID: 39354970
- PMCID: PMC11440973
- DOI: 10.3389/fnume.2022.825891
Normal Variants and Pitfalls of 18F-FDG PET/CT Imaging in Pediatric Oncology
Abstract
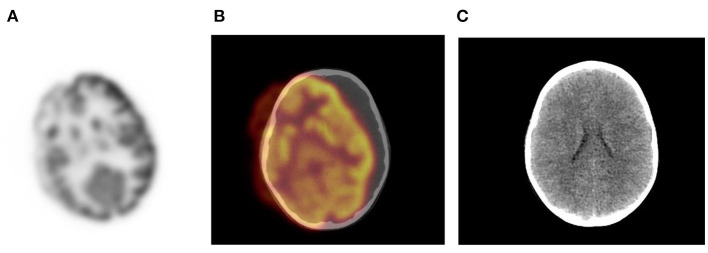
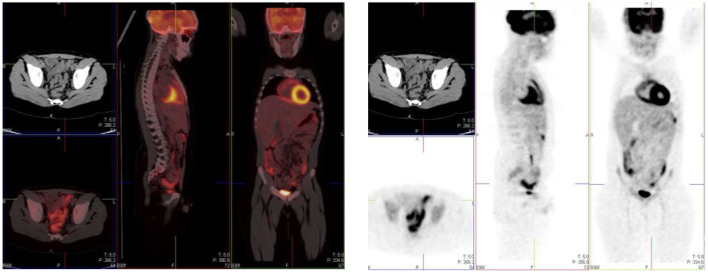
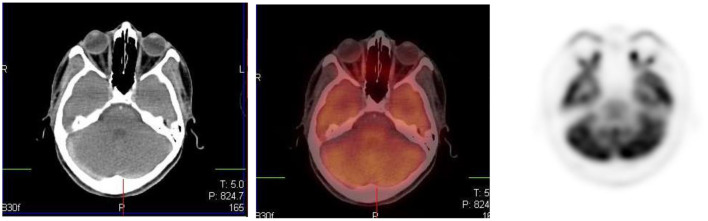
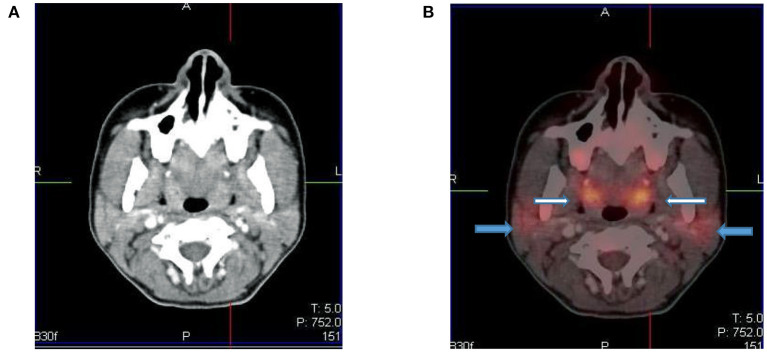
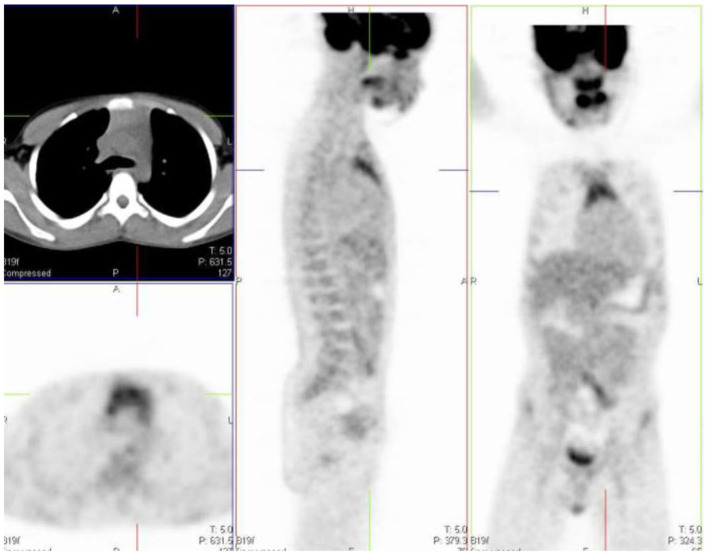
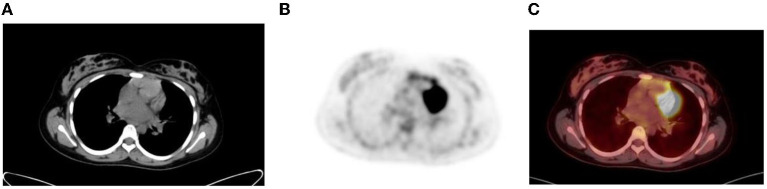
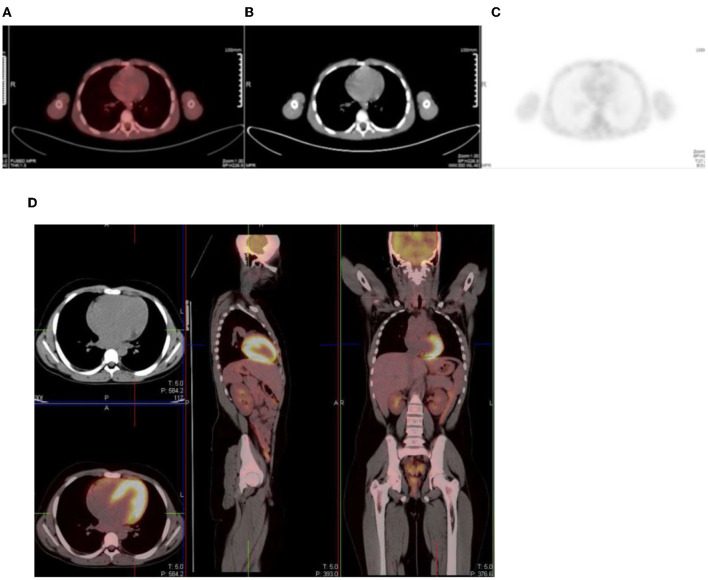
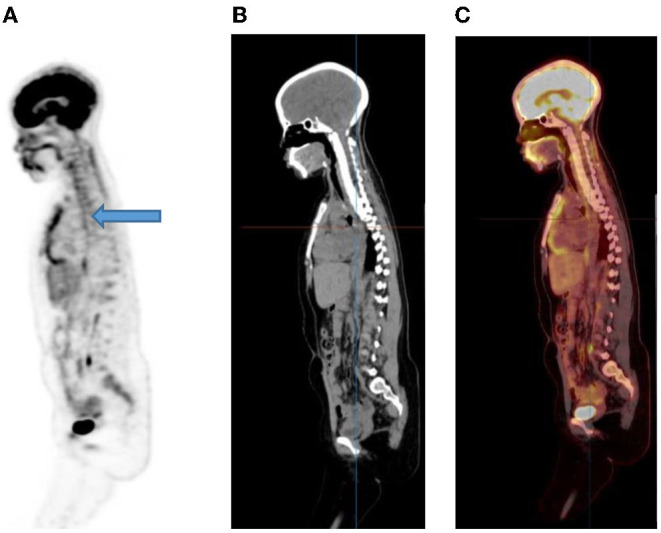
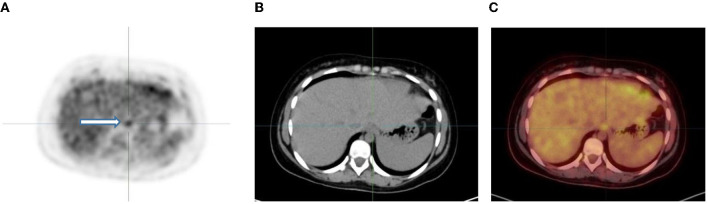
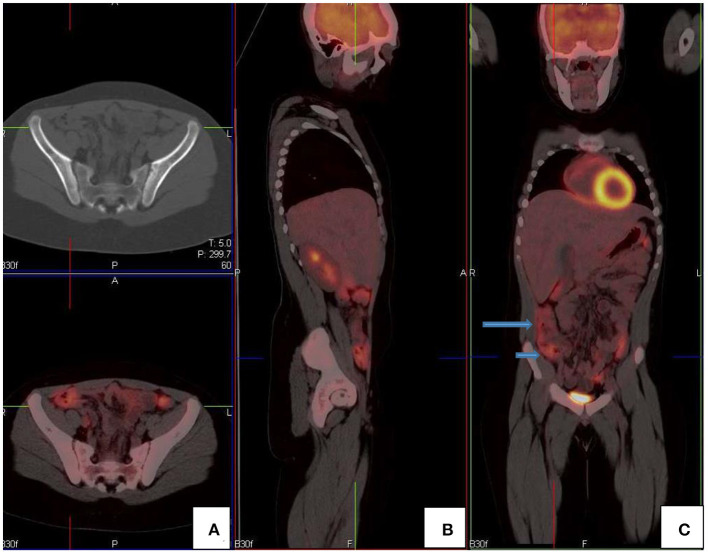
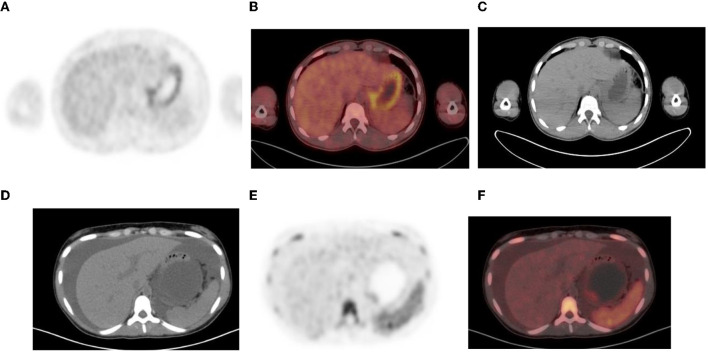
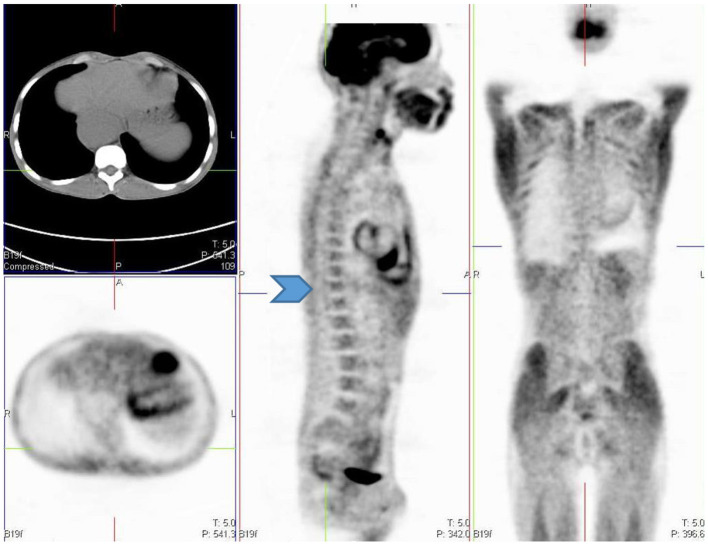
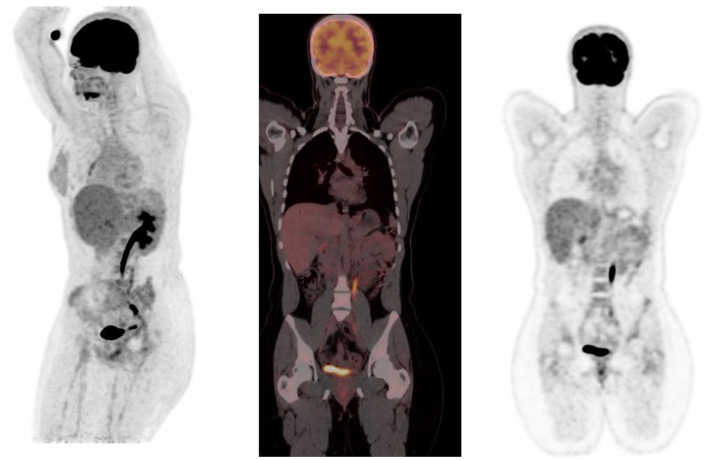
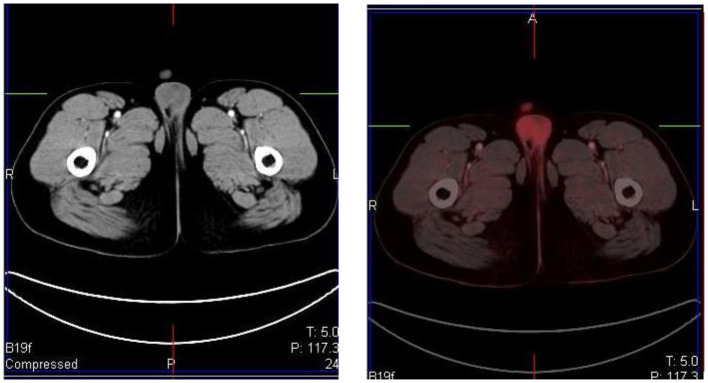
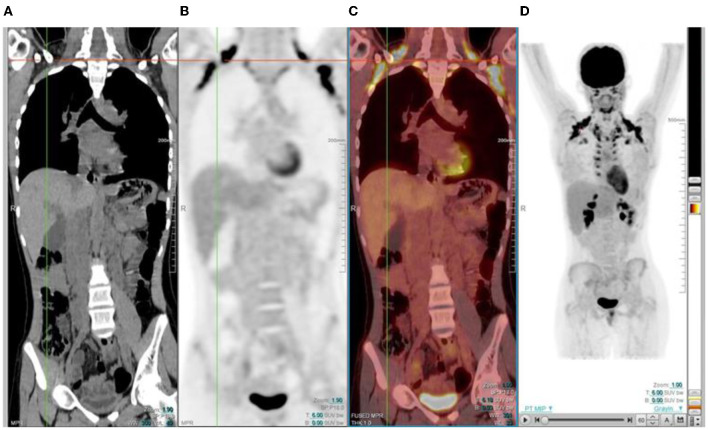
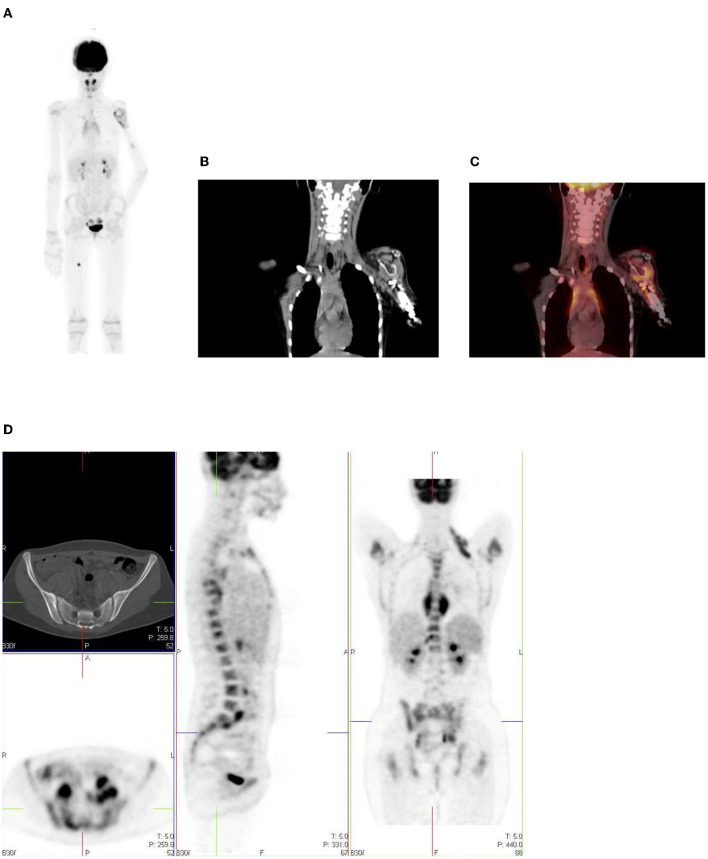
Positron emission tomography (PET) with 2-[fluorine-18] fluoro-2- deoxy-D-glucose (FDG) is a well-established modality that is used in adult oncologic imaging. Its use in pediatric oncology has increased over time. It enables increased diagnostic accuracy due to the combination of functional and morphologic imaging, resulting in optimal patient management. However, the clinician should be aware that the normal distribution of FDG uptake in children differs from adults. Also, even though FDG is used widely in oncology, it is not tumor specific. Uptake of FDG may be seen in numerous benign conditions, including inflammation, infection, and trauma. Proper interpretation of pediatric FDG PET/CT studies requires knowledge of the normal distribution of FDG uptake in children, and an insight into the physiologic variants, benign lesions, and PET/CT related artifacts. Understanding the potential causes of misinterpretation increases the confidence of image interpretation, reduce the number of unnecessary follow-up studies, optimize treatment and more importantly, reduce the radiation exposure to the patient. We review and discuss the physiological distribution of FDG uptake in children, the variation in distribution, lesions that are benign that could be misinterpreted as malignancy, and the various artifacts associated with PET/CT performed in pediatric oncology patients. We add a pictorial illustration to prompt understanding and familiarity of the above-mentioned patterns. Therefore, we believe that this review will assist in reducing possible mistakes by reading physicians and prevent incorrect interpretation.
Keywords: 18F-FDG PET/CT; normal variant; oncology; pediatric nuclear medicine; physiological.
Copyright © 2022 Purbhoo and Vangu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources