

The High-Sensitivity C-Reactive Protein to High-Density Lipoprotein Cholesterol Ratio and the Risk of Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Intervention
- PMID: 39355575
- PMCID: PMC11440391
- DOI: 10.31083/j.rcm2509338
The High-Sensitivity C-Reactive Protein to High-Density Lipoprotein Cholesterol Ratio and the Risk of Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Intervention
Abstract
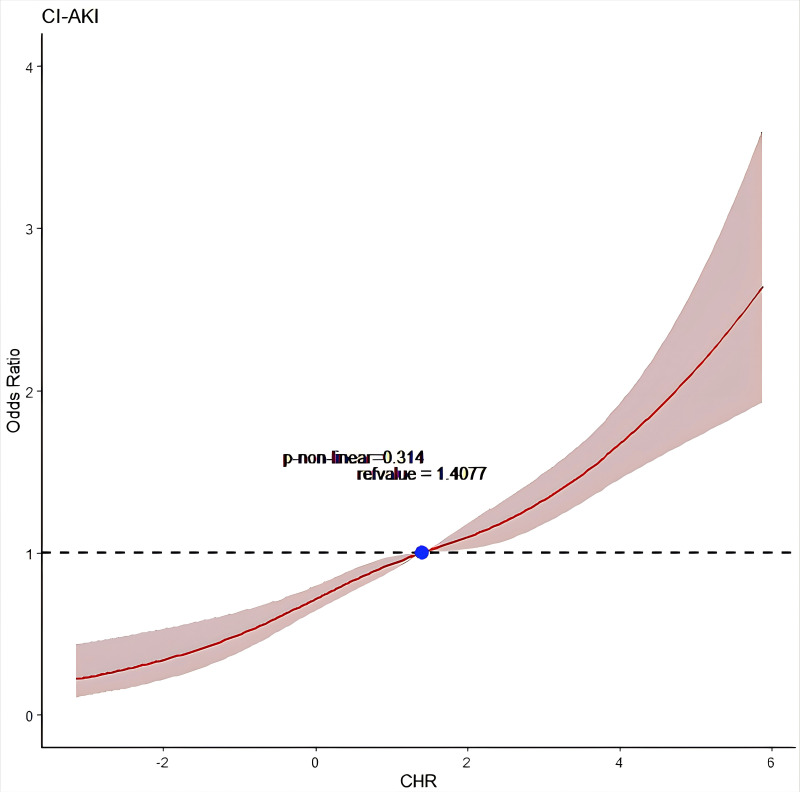
Background: The high-sensitivity C-reactive protein to high-density lipoprotein cholesterol ratio (CHR) is a novel biomarker associated with coronary artery disease (CAD) risk. This study aimed to analyze the relationship between CHR and contrast-induced acute kidney injury (CI-AKI).
Methods: This retrospective cross-sectional research included 10,917 individuals who underwent PCI. CI-AKI was diagnosed using the Kidney Disease: Improving Global Outcomes (KIDIGO) standard. Univariate and multivariable logistic regression analyses were conducted to examine the association between CHR and CI-AKI, followed by a receiver operating characteristic (ROC) curve of participants to assess the clinical diagnostic performance of CHR on CI-AKI.
Results: A total of 1037 patients (9.50%) developed CI-AKI after PCI. The age of individuals averaged 64.1 ± 11.1 years old, with 2511 females (23.0%). A multivariate logistic regression study revealed that higher CHR levels were linked to higher CI-AKI incidence rates ([Q4 vs. Q1]: odds ratio (OR) = 1.89, 95% confidence interval (CI) [1.42 to 2.54], p < 0.001). A restricted cubic spline analysis revealed a linear association between CHR and CI-AKI. ROC analysis indicated that CHR was an excellent predictor of CI-AKI (area under ROC curve = 0.606, 95% CI [0.588 to 0.624]).
Conclusions: A high CHR level is strongly associated with increased CI-AKI incidence, suggesting that CHR may be an independent risk factor for CI-AKI.
Clinical trial registration: NCT05050877. https://clinicaltrials.gov/study/NCT05050877?tab=results.
Keywords: biological indicators; contrast-induced acute kidney injury; high-density lipoprotein cholesterol; high-sensitivity C-reactive protein.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
LDL cholesterol as a novel risk factor for contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention.Atherosclerosis. 2014 Dec;237(2):453-9. doi: 10.1016/j.atherosclerosis.2014.10.022. Epub 2014 Oct 17. Atherosclerosis. 2014. PMID: 25463073
-
Predictive Value of Neutrophil to High-Density Lipoprotein Ratio for Contrast-Induced Acute Kidney Injury for Patients with Acute Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention.Rev Cardiovasc Med. 2023 Feb 10;24(2):59. doi: 10.31083/j.rcm2402059. eCollection 2023 Feb. Rev Cardiovasc Med. 2023. PMID: 39077413 Free PMC article.
-
Preprocedural SII Combined with High-Sensitivity C-Reactive Protein Predicts the Risk of Contrast-Induced Acute Kidney Injury in STEMI Patients Undergoing Percutaneous Coronary Intervention.J Inflamm Res. 2022 Jun 25;15:3677-3687. doi: 10.2147/JIR.S370085. eCollection 2022. J Inflamm Res. 2022. PMID: 35783247 Free PMC article.
-
Remote Ischemic Conditioning for Preventing Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions/Coronary Angiography: A Meta-Analysis of Randomized Controlled Trials.J Cardiovasc Pharmacol Ther. 2016 Jan;21(1):53-63. doi: 10.1177/1074248415590197. Epub 2015 Jun 24. J Cardiovasc Pharmacol Ther. 2016. PMID: 26112028 Review.
-
Risk of contrast-induced acute kidney injury in ST-elevation myocardial infarction patients undergoing multi-vessel intervention-meta-analysis of randomized trials and risk prediction modeling study using observational data.Catheter Cardiovasc Interv. 2017 Aug 1;90(2):205-212. doi: 10.1002/ccd.26928. Epub 2017 Jan 23. Catheter Cardiovasc Interv. 2017. PMID: 28112470 Review.
Cited by
-
Association between high-sensitivity C-reactive protein and diabetic nephropathy: a systematic review and meta-analysis.BMC Nephrol. 2025 Jul 26;26(1):418. doi: 10.1186/s12882-025-04358-y. BMC Nephrol. 2025. PMID: 40713563 Free PMC article.
-
Association of Three Novel Inflammatory Markers: Lymphocyte to HDL-C Ratio, High-Sensitivity C-Reactive Protein to HDL-C Ratio and High-Sensitivity C-Reactive Protein to Lymphocyte Ratio With Metabolic Syndrome.Endocrinol Diabetes Metab. 2024 May;7(3):e00479. doi: 10.1002/edm2.479. Endocrinol Diabetes Metab. 2024. PMID: 38590230 Free PMC article.
References
-
- McCullough PA. Contrast-induced acute kidney injury. Journal of the American College of Cardiology . 2008;51:1419–1428. - PubMed
-
- Fähling M, Seeliger E, Patzak A, Persson PB. Understanding and preventing contrast-induced acute kidney injury. Nature Reviews . 2017;13:169–180. Nephrology. - PubMed
-
- McCullough PA, Choi JP, Feghali GA, Schussler JM, Stoler RM, Vallabahn RC, et al. Contrast-Induced Acute Kidney Injury. Journal of the American College of Cardiology . 2016;68:1465–1473. - PubMed
-
- McCullough PA, Adam A, Becker CR, Davidson C, Lameire N, Stacul F, et al. Epidemiology and prognostic implications of contrast-induced nephropathy. The American Journal of Cardiology . 2006;98:5K–13K. - PubMed
-
- Stacul F, van der Molen AJ, Reimer P, Webb JAW, Thomsen HS, Morcos SK, et al. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. European Radiology . 2011;21:2527–2541. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
