

Advances in the Management of Spontaneous Coronary Artery Dissection (SCAD): A Comprehensive Review
- PMID: 39355597
- PMCID: PMC11440404
- DOI: 10.31083/j.rcm2509345
Advances in the Management of Spontaneous Coronary Artery Dissection (SCAD): A Comprehensive Review
Abstract
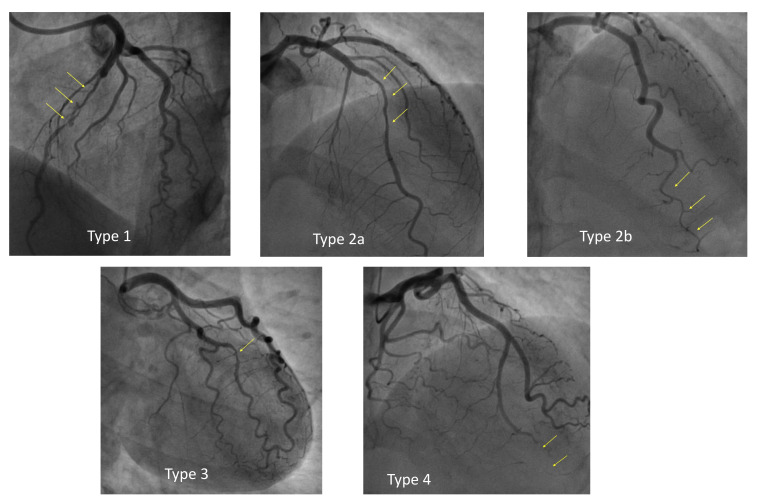
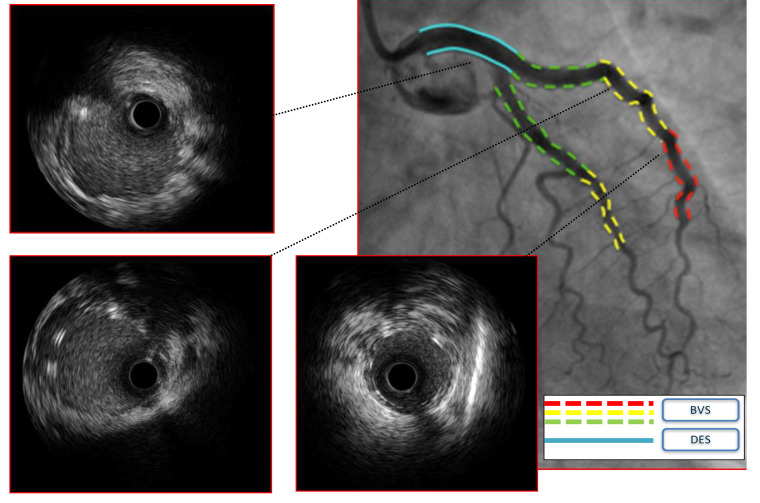
Spontaneous coronary artery dissection (SCAD) is a rare but significant cause of acute coronary syndrome (ACS), primarily affecting young women, often during pregnancy. Despite its rarity, SCAD poses challenges due to limited evidence on management strategies. This review examines the current state of art of SCAD management, integrating interventional and clinical insights from recent studies. The epidemiology of SCAD is related to its elusive nature, representing only a small fraction of ACS cases, while certainly underestimated. Proposed risk factors include genetic, hormonal, and environmental influences. Angiographic classification may help in SCAD diagnosis, but confirmation often relies on intracoronary imaging. Conservative management constitutes the primary approach, showing efficacy in most cases, although optimal antiplatelet therapy (APT) remains debated due to bleeding risks associated with intramural hematoma. Revascularization is reserved for high-risk cases, guided by angiographic and clinical criteria, with a focus on restoring flow rather than resolving dissection. Interventional strategies emphasize a minimalist approach to reduce complications, utilizing techniques such as balloon dilation and stent placement tailored to individual cases. Long-term outcomes highlight the risk of recurrence, necessitating vigilant follow-up and arrhythmic risk assessment, particularly in patients presenting with ventricular arrhythmias. In conclusion, SCAD management always represents a challenge for the physician, both from a clinical and interventional point of view. Recent clinical evidence and a multidisciplinary approach are vital for optimizing patient outcomes and preventing recurrence. This review offers a concise framework for navigating the complexities of SCAD management in clinical practice and proposes an algorithm for its management.
Keywords: acute coronary syndrome (ACS); antiplatelet therapy; fibromuscular dysplasia; myocardial infarction; percutaneous coronary intervention (PCI); pregnancy-associated; spontaneous coronary artery dissection (SCAD); women.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest. Fabrizio D’Ascenzo is serving as one of the Editorial Board members of this journal. We declare that Fabrizio D’Ascenzo had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Dimitris Tousoulis.
Figures




References
-
- Boulmpou A, Kassimis G, Zioutas D, Meletidou M, Mouselimis D, Tsarouchas A, et al. Spontaneous Coronary Artery Dissection (SCAD): Case Series and Mini Review. Cardiovascular Revascularization Medicine: Including Molecular Interventions . 2020;21:1450–1456. - PubMed
-
- Elkayam U, Jalnapurkar S, Barakkat MN, Khatri N, Kealey AJ, Mehra A, et al. Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation . 2014;129:1695–1702. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
