

F-18 FDG PET/CT Imaging in Normal Variants, Pitfalls and Artifacts in the Abdomen and Pelvis
- PMID: 39355643
- PMCID: PMC11440875
- DOI: 10.3389/fnume.2021.826109
F-18 FDG PET/CT Imaging in Normal Variants, Pitfalls and Artifacts in the Abdomen and Pelvis
Abstract
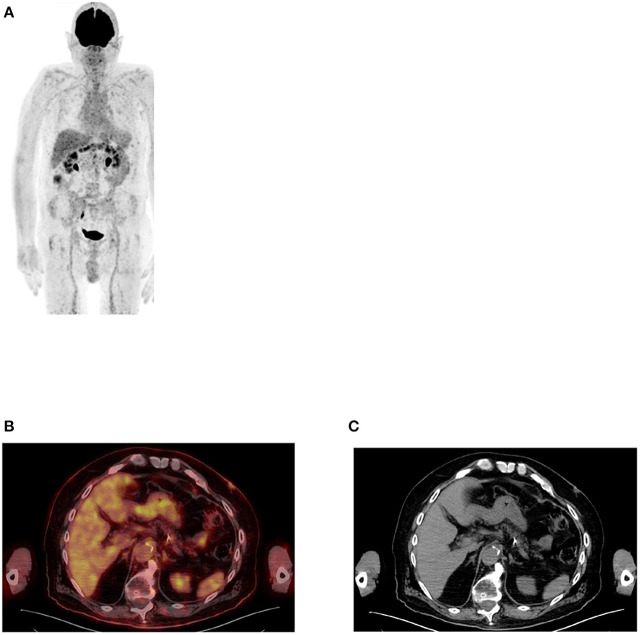
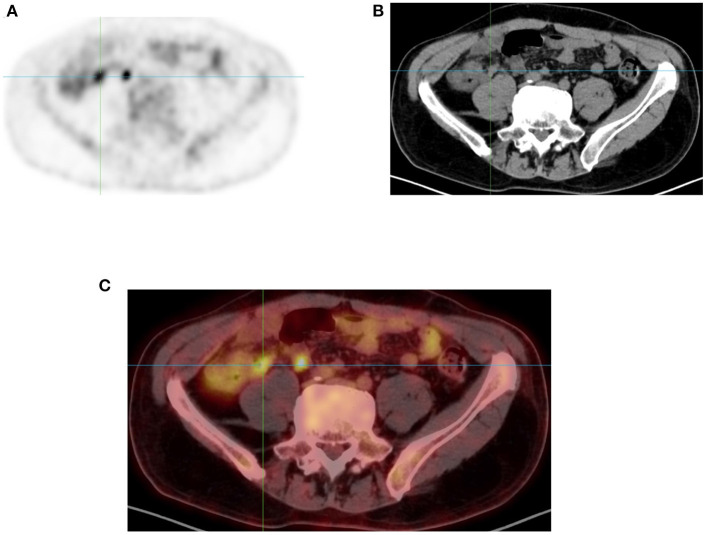
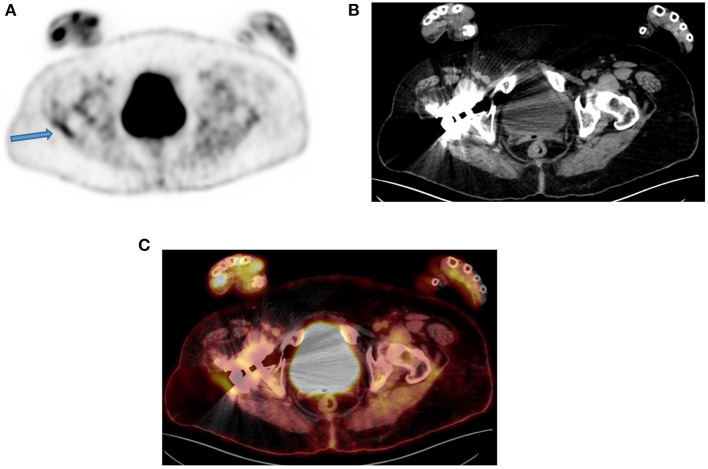
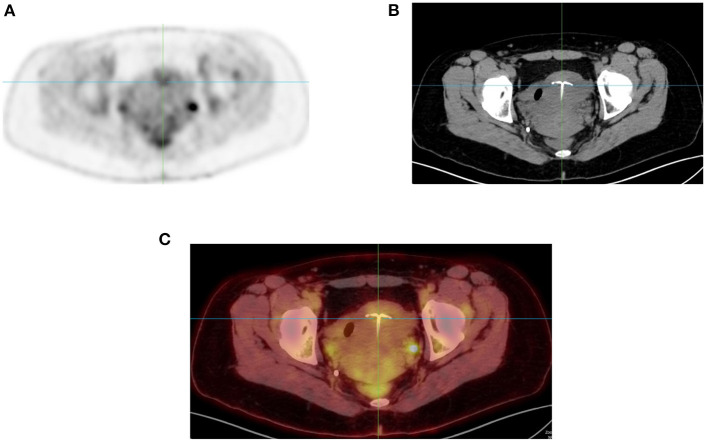
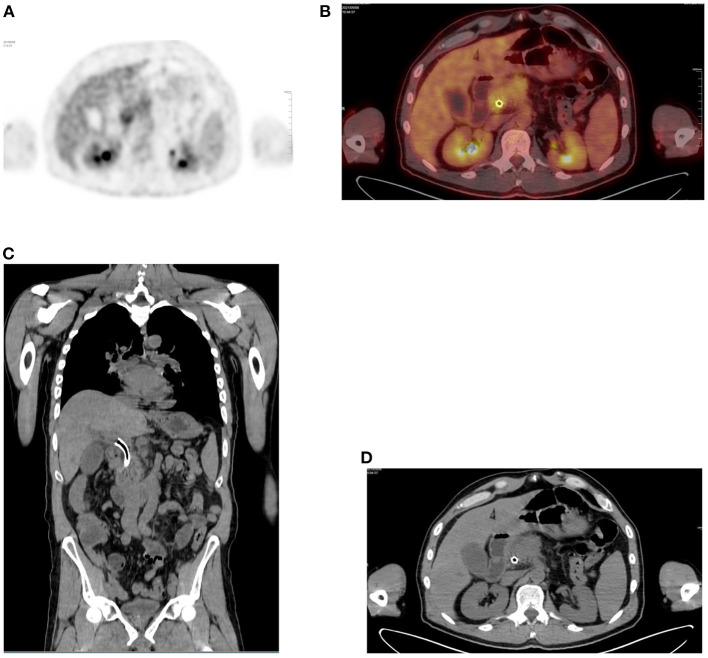
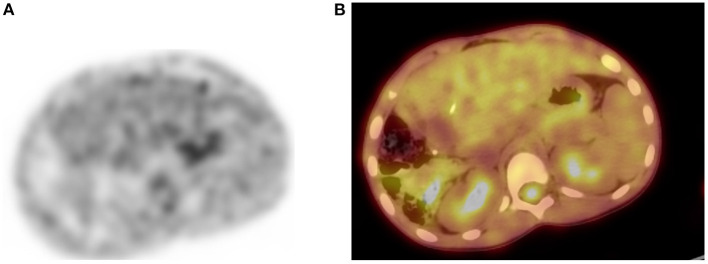
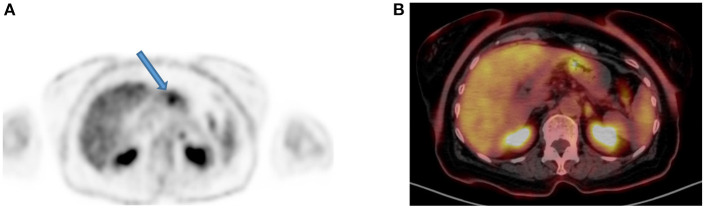
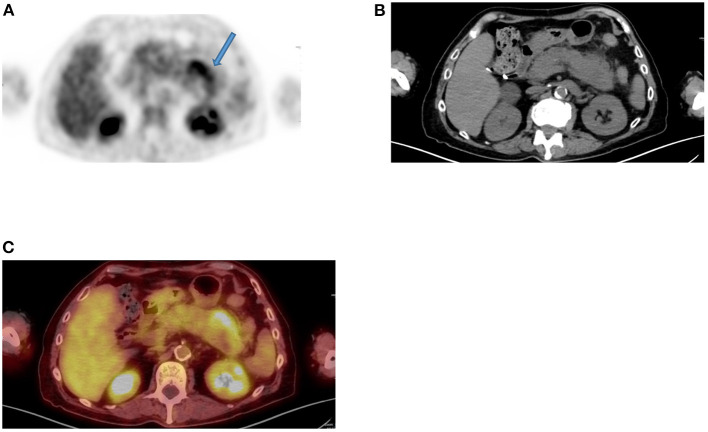
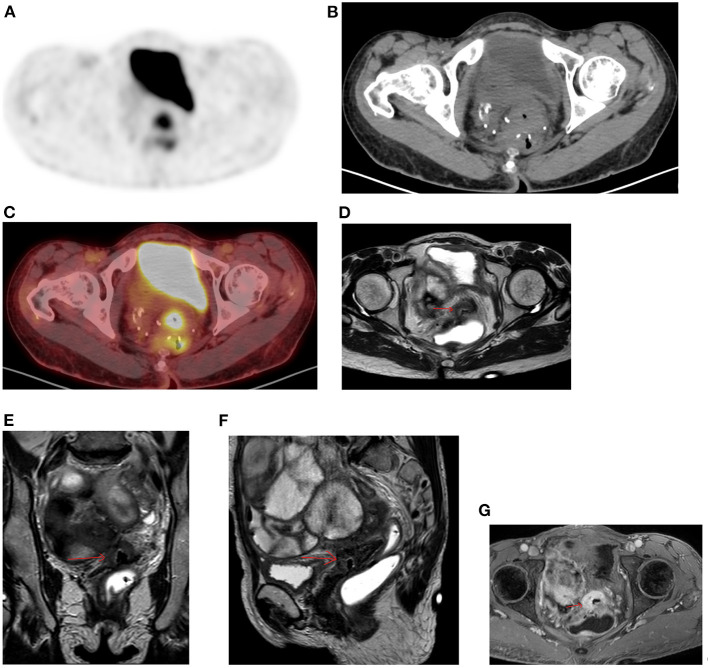
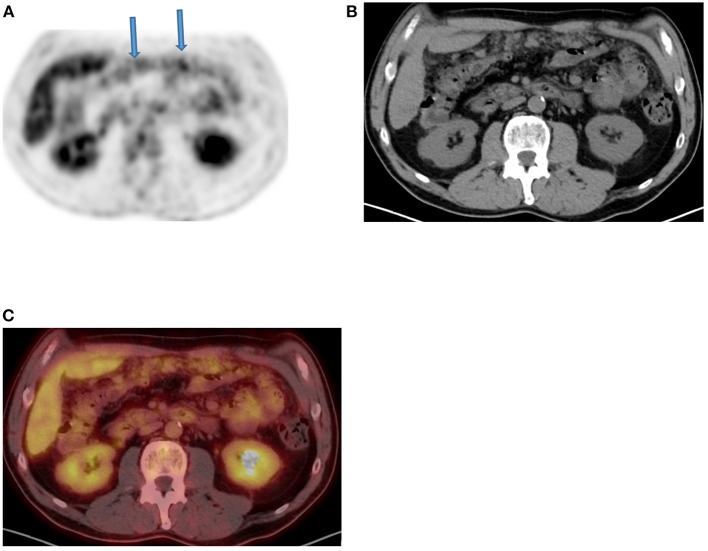
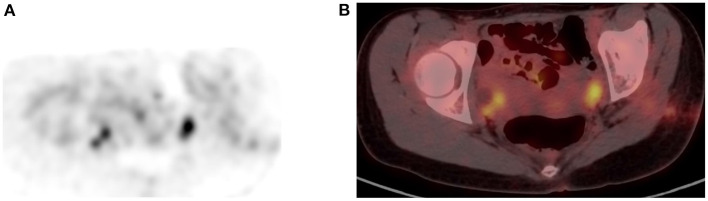
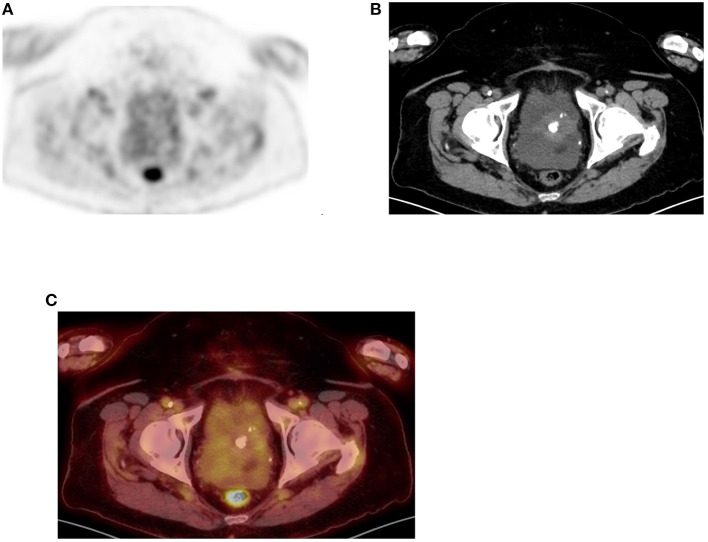
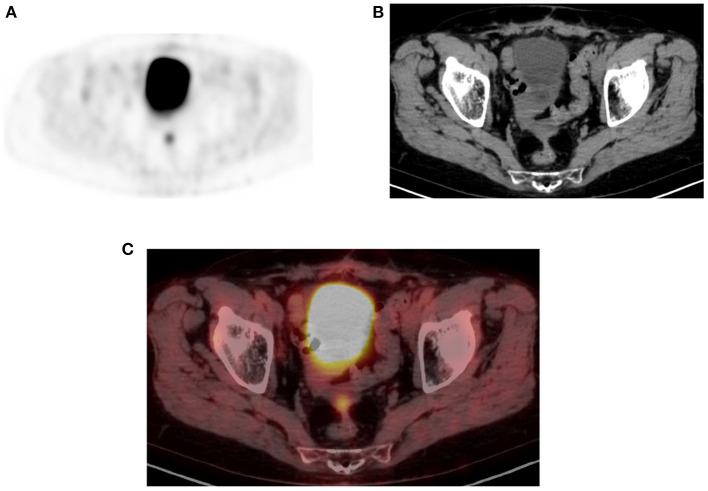
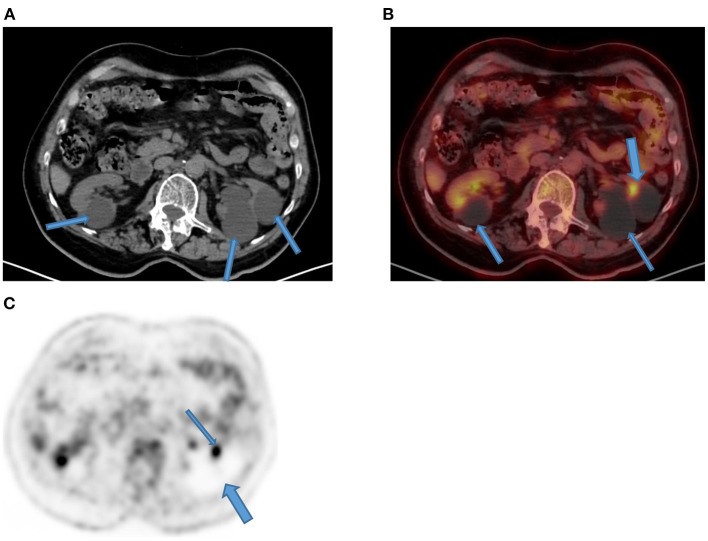
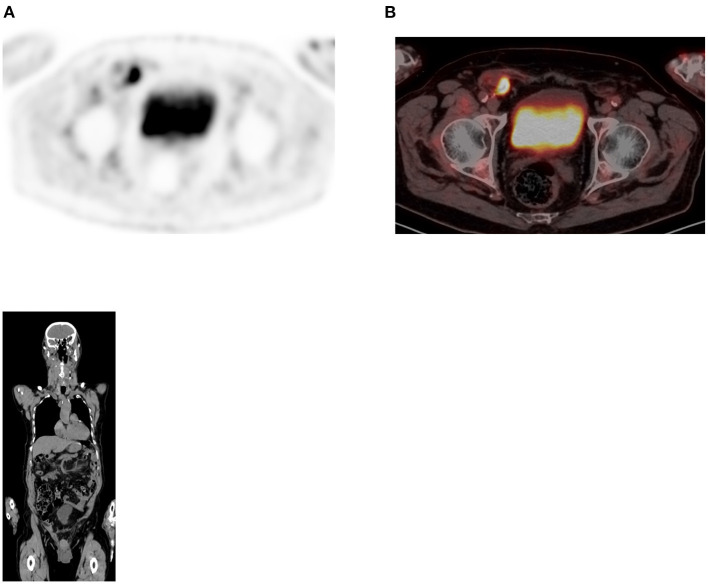
Since its introduction into clinical practice, multimodality imaging has revolutionized diagnostic imaging for both oncologic and non-oncologic pathologies. 18F-fluorodeoxyglucose (18F-FDG) PET/CT imaging which takes advantage of increased anaerobic glycolysis that occurs in tumor cells (Warburg effect) has gained significant clinical relevance in the management of most, if not all oncologic conditions. Because FDG is taken by both normal and abnormal tissues, PET/CT imaging may demonstrate several normal variants and imaging pitfalls. These may ultimately impact disease detection and diagnostic accuracy. Imaging specialists (nuclear medicine physicians and radiologists) must demonstrate a thorough understanding of normal and physiologic variants in the distribution of 18F-FDG; including potential imaging pitfalls and technical artifacts to minimize misinterpretation of images. The normal physiologic course of 18F-FDG results in a variable degree of uptake in the stomach, liver, spleen, small and large bowel. Urinary excretion results in renal, ureteric, and urinary bladder uptake. Technical artifacts can occur due to motion, truncation as well as the effects of contrast agents and metallic hardware. Using pictorial illustrations, this paper aims to describe the variants of physiologic 18F-FDG uptake that may mimic pathology as well as potential benign conditions that may result in misinterpretation of PET/CT images in common oncologic conditions of the abdomen and pelvis.
Keywords: FDG; PET/CT; abdomen; pelvis; pitfalls; variants.
Copyright © 2022 Vangu and Momodu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Lin E, Alavi A. PET and PET/CT- A Clinical Guide. 3rd ed. New York, NY: Thieme; (2019).
Publication types
LinkOut - more resources
Full Text Sources