

Prolonged 120-h meropenem antibiotic prophylaxis in radical cystectomy compared to 24h standard antibiotic prophylaxis: Final analysis of the randomized clinical trial
- PMID: 39355793
- PMCID: PMC11441018
- DOI: 10.1080/20905998.2024.2373399
Prolonged 120-h meropenem antibiotic prophylaxis in radical cystectomy compared to 24h standard antibiotic prophylaxis: Final analysis of the randomized clinical trial
Abstract
Background: Standard 24-h antibiotic prophylaxis (AP) is widely employed to minimize the risk of infection complications (ICs) within 30 days following a radical cystectomy (RC). However, a considerable variety of prophylaxis protocols do not prevent a high ICs rate after surgery (37-67%). Therefore, antibiotic's type and its duration are still controversial for AP.(.
Objective: To compare standard 24-h AP with a prolonged 120-h regimen in a multicenter randomized clinical trial.
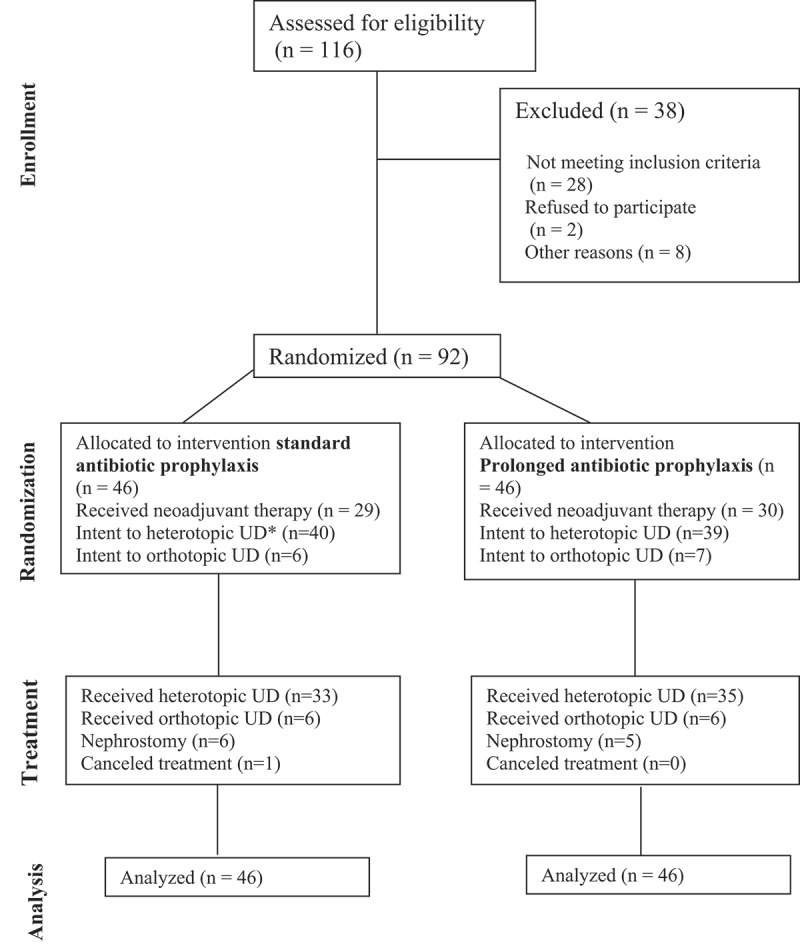
Methods: Patients were randomized in a 1:1 ratio to standard 24-h AP regimen (Group A) versus the prolonged meropenem AP 120-h (Group B). The primary endpoint was an event rate defined as the frequency of ICs within 30 days. The secondary endpoint were biomarker's analysis and antibiotic re-administration rate (ArAR).
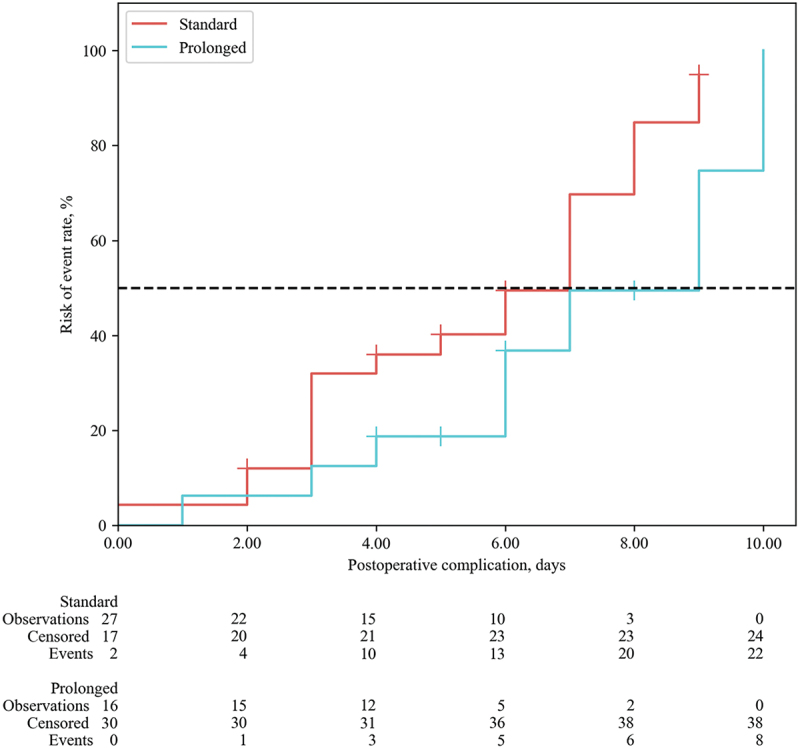
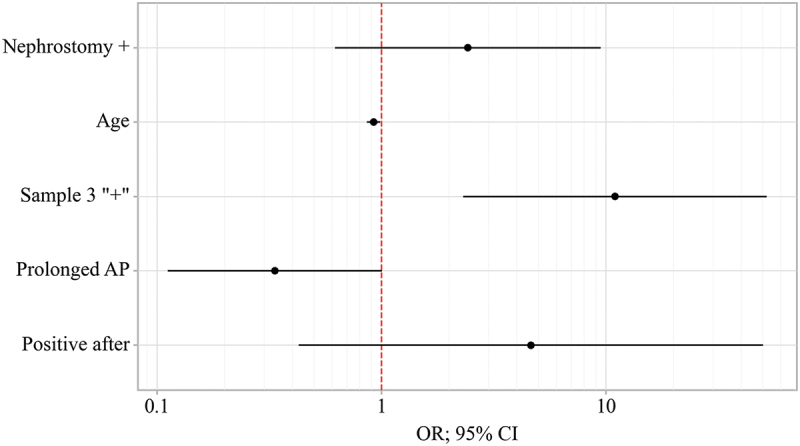
Results: A total of 92 patients were enrolled. The Clavien-Dindo complications rate did not differ between the groups (p = 0.065), however the overall complication rate was higher in Group A (63.0% vs. 34.8%, p = 0.007). The infection complication rate was 2.75 times higher in the standard antibiotic prophylaxis group: 47.8% compared to 17.4% cases in Group B (p = 0.002). The new prolonged antibiotic regimen decreased the risk of ICs (OR 0.23; 95% CI 0.08-.598; p = 0.003).The event-free survival for ICs of clinical interest in group A was 7.00 days and in group B was 9.00 days (HR = 0.447; 0.191-1.050, p = 0.065). The ArAR was higher in Group A -47.8%, while in Group B it was only in 17.4% of the cases. The incidence of bacteriuria before RC was the same between groups (p = 0.666), however, after stent removal the risk of a positive culture was lower in group B (RR = 0.64; 95% CI 0.37-1.08; p = 0.05).
Conclusions: The administration AP over 120-h appears to be safe and feasible, demonstrating a reduction in the total number of complications and ArAR. Trial registration in Clinical Trials: NCT05392634.Trial registration in Clinical Trials: NCT05392634.
Keywords: Radical cystectomy; antibiotic prophylaxis; carbapenemase; infection complications; surgical site infection.
© 2024 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Gontero P. Guidelines on mon-muscle-invasive bladder cancer (Ta, T1 and CIS). In: EAU Guidelines published at the 38th Annual Congress Milan; Arnhem, the Netherlands. European Associaton of Urology Guidelines Office; 2023.
-
- Nosov AK, Reva SA, Dzhalilov IB, et al. Radical cystectomy for bladder cancer: сomparison of early surgical complications during laparoscopic, open-access, and video-assisted surgery. Oncourology. 2015;11(3):71–78 (In Russ.). doi: 10.17650/1726-9776-2015-11-3-71-78 - DOI
Associated data
LinkOut - more resources
Full Text Sources
Medical