

Photon-counting detector computed tomography in cardiac imaging
- PMID: 39356451
- PMCID: PMC11502613
- DOI: 10.1007/s12471-024-01904-5
Photon-counting detector computed tomography in cardiac imaging
Abstract
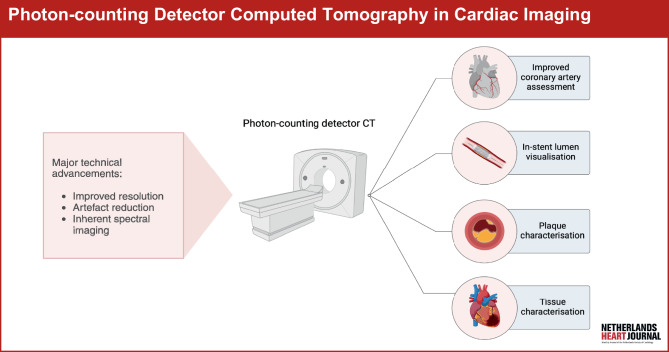
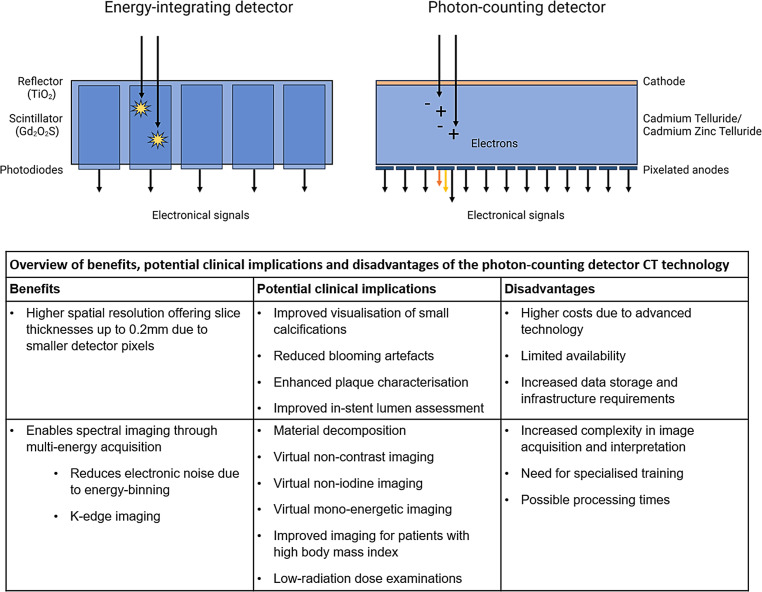
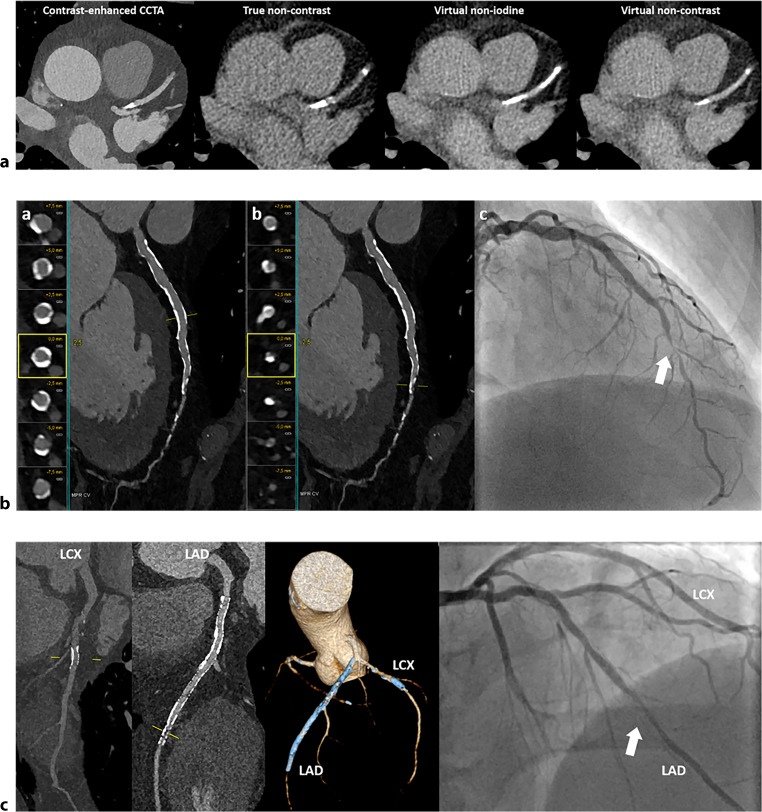
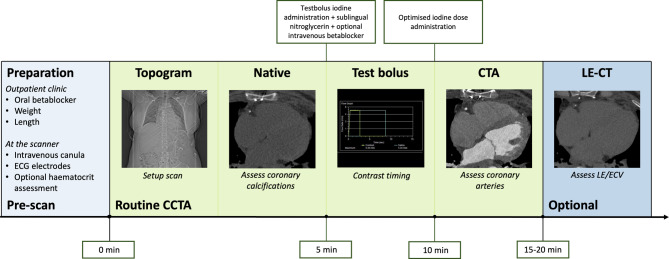
Photon-counting detector computed tomography (PCD-CT) has emerged as a revolutionary technology in CT imaging. PCD-CT offers significant advancements over conventional energy-integrating detector CT, including increased spatial resolution, artefact reduction and inherent spectral imaging capabilities. In cardiac imaging, PCD-CT can offer a more accurate assessment of coronary artery disease, plaque characterisation and the in-stent lumen. Additionally, it might improve the visualisation of myocardial fibrosis through qualitative late enhancement imaging and quantitative extracellular volume measurements. The use of PCD-CT in cardiac imaging holds significant potential, positioning itself as a valuable modality that could serve as a one-stop-shop by integrating both angiography and tissue characterisation into a single examination. Despite its potential, large-scale clinical trials, standardisation of protocols and cost-effectiveness considerations are required for its broader integration into clinical practice. This narrative review provides an overview of the current literature on PCD-CT regarding the possibilities and limitations of cardiac imaging.
Keywords: Angiography; Cardiac imaging techniques; Coronary artery disease; Tomography, X‑ray computed.
© 2024. The Author(s).
Conflict of interest statement
M.W. Smulders: Speakers fee ESC highlights ’22 and ’23—Daiichi Sankyo Europe. Academic Grant by Maastricht UMC+. R.P.J. Budde: Institutional support to EMC by Siemens and Heartflow. Speakers fee Bayer. A. Hirsch: Editor for Netherlands Heart Journal. Received a research grant and consultancy fees from GE Healthcare and speaker fees from GE Healthcare and Bayer. He is also a member of the medical advisory board of Medis Medical Imaging Systems and was MRI corelab supervisor of Cardialysis BV until 2022. C. Mihl: Speakers bureau Bayer Healthcare. Academic Grant by Maastricht UMC+. MJ.D.K. Lemmens and S.P. Sharma declare that they have no competing interests.
Figures
References
-
- Willemink MJ, Persson M, Pourmorteza A, Pelc NJ, Fleischmann D. Photon-counting CT: technical principles and clinical prospects. Radiology. 2018;289:293–312. - PubMed
-
- van der Bie J, van Straten M, Booij R, et al. Photon-counting CT: review of initial clinical results. Eur J Radiol. 2023;163:110829. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
