

Trajectory of Cognitive Decline Before and After Stroke in 14 Population Cohorts
- PMID: 39356504
- PMCID: PMC11447567
- DOI: 10.1001/jamanetworkopen.2024.37133
Trajectory of Cognitive Decline Before and After Stroke in 14 Population Cohorts
Abstract
Importance: Poststroke cognitive impairment is common, but the cognitive trajectory following a first stroke, relative to prestroke cognitive function, remains unclear.
Objective: To map the trajectory of cognitive function before any stroke and after stroke in global cognition and in 4 cognitive domains, as well as to compare the cognitive trajectory prestroke in stroke survivors with the trajectory of individuals without incident stroke over follow-up.
Design, setting, and participants: The study used harmonized and pooled data from 14 population-based cohort studies included in the Cohort Studies of Memory in an International Consortium collaboration. These studies were conducted from 1993 to 2019 across 11 countries among community-dwelling older adults without a history of stroke or dementia. For this study, linear mixed-effects models were used to estimate trajectories of cognitive function poststroke relative to a stroke-free cognitive trajectory. The full model adjusted for demographic and vascular risk factors. Data were analyzed from July 2022 to March 2024.
Exposure: Incident stroke.
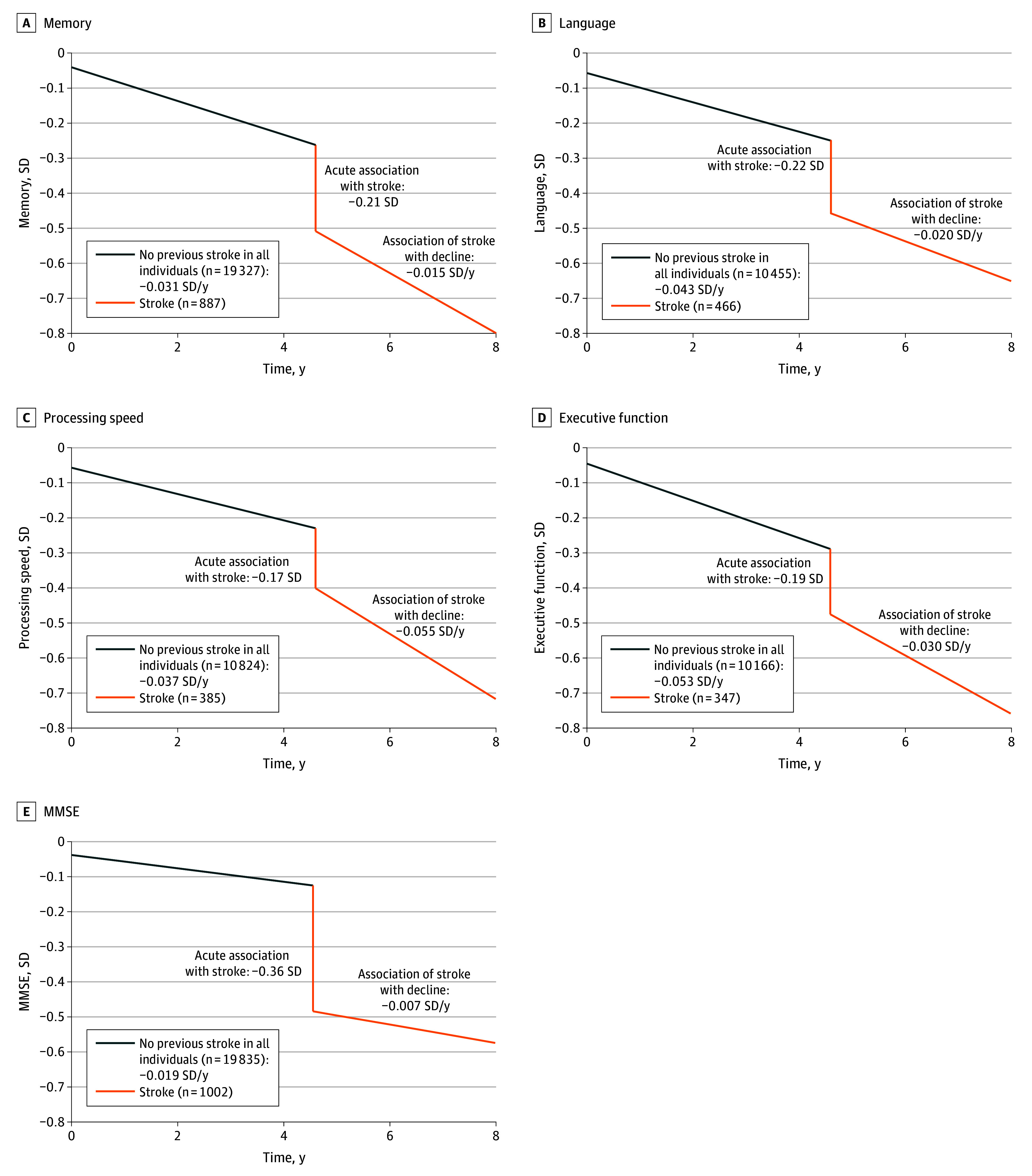
Main outcomes and measures: The primary outcome was global cognition, defined as the standardized average of 4 cognitive domains (language, memory, processing speed, and executive function). Cognitive domain scores were formed by selecting the most commonly administered test within each domain and standardizing the scores.
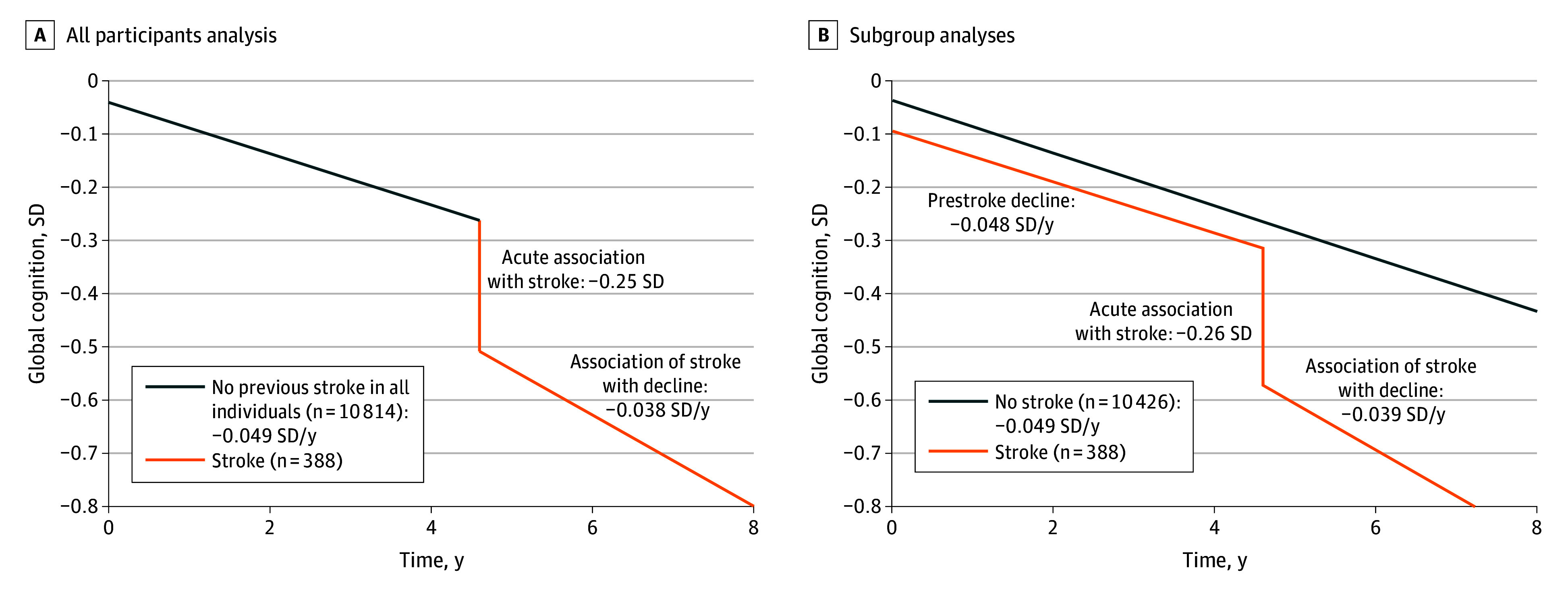
Results: The study included 20 860 participants (12 261 [58.8%] female) with a mean (SD) age of 72.9 (8.0) years and follow-up of 7.51 (4.2) years. Incident stroke was associated with a substantial acute decline in global cognition (-0.25 SD; 95% CI, -0.33 to -0.17 SD), the Mini-Mental State Examination, and all cognitive domains (ranging from -0.17 SD to -0.22 SD), as well as accelerated decline in global cognition (-0.038 SD per year; 95% CI, -0.057 to -0.019 SD per year) and all domains except memory (ranging from -0.020 to -0.055 SD per year), relative to a stroke-free cognitive trajectory. There was no significant difference in prestroke slope in stroke survivors compared with the rate of decline in individuals without stroke in all cognitive measures. The mean rate of decline without a previous stroke was -0.049 SD per year (95% CI, -0.051 to -0.047 SD) in global cognition.
Conclusions and relevance: In this cohort study using pooled data from 14 cohorts, incident stroke was associated with acute and accelerated long-term cognitive decline in older stroke survivors.
Conflict of interest statement
Figures
Comment in
-
Understanding Cognitive Decline After Stroke in the Acute Setting.JAMA Netw Open. 2024 Oct 1;7(10):e2437145. doi: 10.1001/jamanetworkopen.2024.37145. JAMA Netw Open. 2024. PMID: 39356510 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
