

Hormonal Contraception and Breast Cancer Risk for Carriers of Germline Mutations in BRCA1 and BRCA2
- PMID: 39356978
- PMCID: PMC11771360
- DOI: 10.1200/JCO.24.00176
Hormonal Contraception and Breast Cancer Risk for Carriers of Germline Mutations in BRCA1 and BRCA2
Abstract
Purpose: It is uncertain whether, and to what extent, hormonal contraceptives increase breast cancer (BC) risk for germline BRCA1 or BRCA2 mutation carriers.
Methods: Using pooled observational data from four prospective cohort studies, associations between hormonal contraceptive use and BC risk for unaffected female BRCA1 and BRCA2 mutation carriers were assessed using Cox regression.
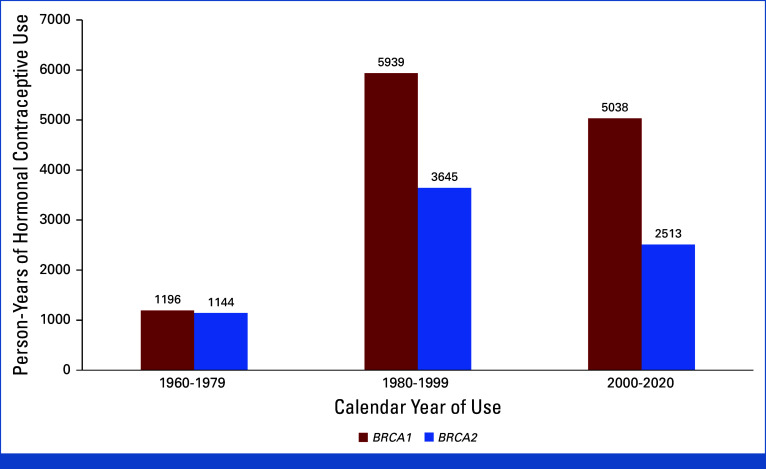
Results: Of 3,882 BRCA1 and 1,509 BRCA2 mutation carriers, 53% and 71%, respectively, had ever used hormonal contraceptives for at least 1 year (median cumulative duration of use, 4.8 and 5.7 years, respectively). Overall, 488 BRCA1 and 191 BRCA2 mutation carriers developed BC during median follow-up of 5.9 and 5.6 years, respectively. Although for BRCA1 mutation carriers, neither current nor past use of hormonal contraceptives for at least 1 year was statistically significantly associated with BC risk (hazard ratio [HR], 1.40 [95% CI, 0.94 to 2.08], P = .10 for current use; 1.16 [0.80 to 1.69], P = .4, 1.40 [0.99 to 1.97], P = .05, and 1.27 [0.98 to 1.63], P = .07 for past use 1-5, 6-10, and >10 years before, respectively), ever use was associated with increased risk (HR, 1.29 [95% CI, 1.04 to 1.60], P = .02). Furthermore, BC risk increased with longer cumulative duration of use, with an estimated proportional increase in risk of 3% (1%-5%, P = .002) for each additional year of use. For BRCA2 mutation carriers, there was no evidence that current or ever use was associated with increased BC risk (HR, 0.70 [95% CI, 0.33 to 1.47], P = .3 and 1.07 [0.73 to 1.57], P = .7, respectively).
Conclusion: Hormonal contraceptives were associated with increased BC risk for BRCA1 mutation carriers, especially if used for longer durations. Decisions about their use in women with BRCA1 mutations should carefully weigh the risks and benefits for each individual.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures


References
-
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. : Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 317:2402-2416, 2017 - PubMed
-
- Iversen L, Sivasubramaniam S, Lee AJ, et al. : Lifetime cancer risk and combined oral contraceptives: The Royal College of General Practitioners’ oral contraception study. Am J Obstet Gynecol 216:580.e1-580.e9, 2017 - PubMed
-
- Collaborative Group on Hormonal Factors in Breast Cancer : Breast cancer and hormonal contraceptives: Collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies. Lancet 347:1713-1727, 1996 - PubMed
-
- Morch LS, Skovlund CW, Hannaford PC, et al. : Contemporary hormonal contraception and the risk of breast cancer. N Engl J Med 377:2228-2239, 2017 - PubMed
-
- Burchardt NA, Eliassen AH, Shafrir AL, et al. : Oral contraceptive use by formulation and breast cancer risk by subtype in the Nurses’ Health study II: A prospective cohort study. Am J Obstet Gynecol 226:821.e1-821.e26, 2022 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
