

Patterns of pain medication usage and self-reported pain in older Irish adults with osteoarthritis: A latent class analysis of data from the Irish Longitudinal Study on Ageing
- PMID: 39358713
- PMCID: PMC11447940
- DOI: 10.1186/s12891-024-07854-8
Patterns of pain medication usage and self-reported pain in older Irish adults with osteoarthritis: A latent class analysis of data from the Irish Longitudinal Study on Ageing
Abstract
Background: This study aimed to identify and describe links between pain medication use and self-reported pain among people aged ≥ 50 years with osteoarthritis (OA) in an Irish population, and to examine the relationships between pain, medication usage and socioeconomic and clinical characteristics.
Methods: Secondary data analysis of wave 1 cross-sectional data from The Irish Longitudinal Study on Ageing (TILDA) was undertaken of 1042 people with self-reported doctor-diagnosed OA. We examined use of medications typically included in OA clinical guidelines, including non-opioid analgesics (e.g. paracetamol), topical and oral non-steroidal anti-inflammatory drugs (NSAIDs), opioids and nutraceuticals. Latent Class Analysis (LCA) was used to identify underlying clinical subgroups based on medication usage patterns, and self-reported pain severity. Multinomial logistic regression was used to explore sociodemographic and clinical characteristic links to latent class membership.
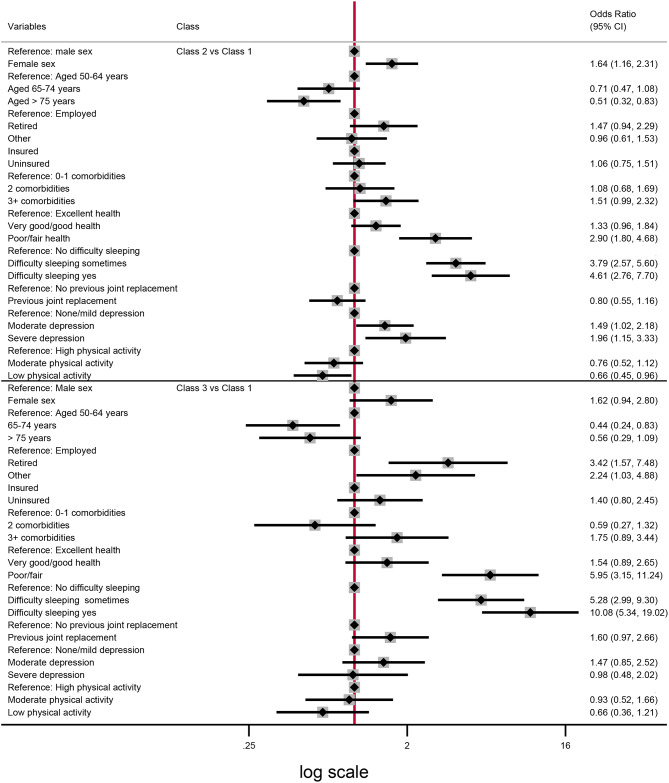
Results: A total of 358 (34.4%) of the 1042 people in this analysis were taking pain medications including oral NSAIDs (17.5%), analgesics (11.4%) and opioids (8.7%). Nutraceutical (glucosamine/chondroitin) use was reported by 8.6% and topical NSAID use reported by 1.4%. Three latent classes were identified: (1) Low medication use/no pain (n = 382, 37%), (2) low medication use/moderate pain (n = 523, 50%) and (3) moderate medication use/high pain (n = 137, 13%). Poorer self-rated health and greater sleep disturbance were associated with classes 2 and 3; depressive symptoms and female gender were associated with class 2, and retirement associated with class 3.
Conclusions: Whilst pain medication use varied with pain severity, different medication types reported broadly aligned with OA guidelines. The two subgroups exhibiting higher pain levels demonstrated poorer self-rated health and greater sleep disturbance.
Keywords: Clinical guidelines; Latent class analysis; Medications; Osteoarthritis; Pain.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Safiri S, Kolahi AA, Smith E, Hill C, Bettampadi D, Mansournia MA, Hoy D, Ashrafi-Asgarabad A, Sepidarkish M, Almasi-Hashiani A, et al. Global, regional and national burden of osteoarthritis 1990–2017: a systematic analysis of the Global Burden of Disease Study 2017. Ann Rheum Dis. 2020;79(6):819–28. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
