

Clinical prognosticators and targets in the immune microenvironment of intrahepatic cholangiocarcinoma
- PMID: 39359389
- PMCID: PMC11445892
- DOI: 10.1080/2162402X.2024.2406052
Clinical prognosticators and targets in the immune microenvironment of intrahepatic cholangiocarcinoma
Abstract
Background: Intrahepatic cholangiocarcinoma (ICC) is a disease with poor prognosis and limited therapeutic options. We investigated the tumor immune microenvironment (TIME) to identify predictors of disease outcome and to explore targets for therapeutic modulation.
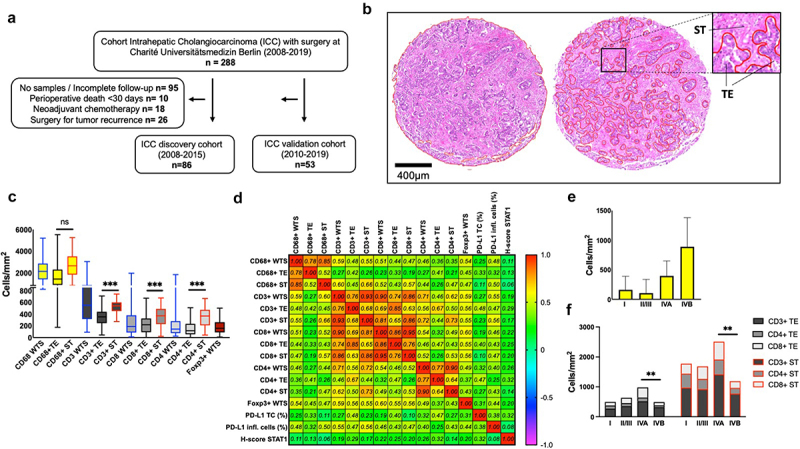
Methods: Liver tissue samples were collected during 2008-2019 from patients (n = 139) diagnosed with ICC who underwent curative intent surgery without neoadjuvant chemotherapy. Samples from the discovery cohort (n = 86) were immunohistochemically analyzed on tissue microarrays (TMAs) for the expression of CD68, CD3, CD4, CD8, Foxp3, PD-L1, STAT1, and p-STAT1 in tumor core and stroma areas. Results were digitally analyzed using QuPath software and correlated with clinicopathological characteristics. For validation of TIME-related biomarkers, we performed multiplex imaging mass cytometry (IMC) in a validation cohort (n = 53).
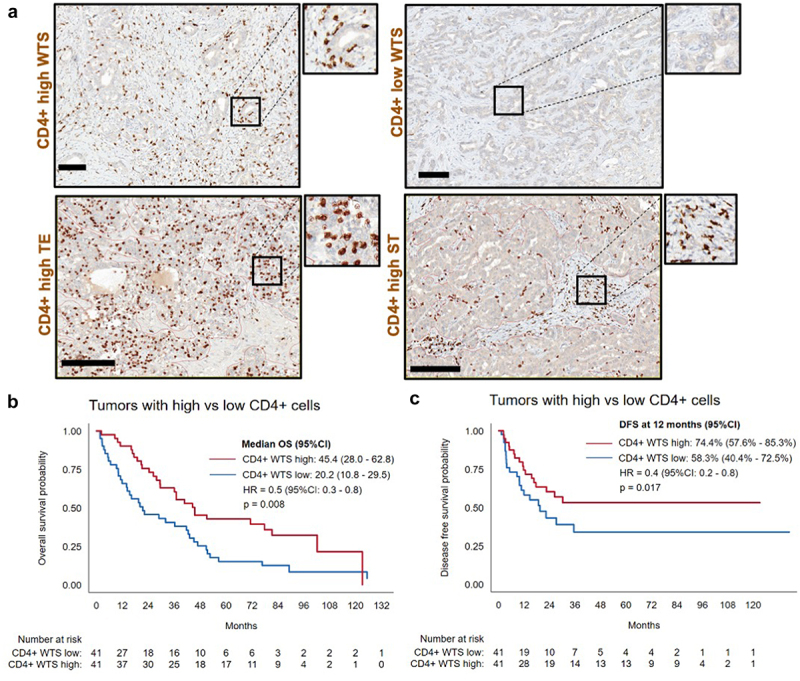
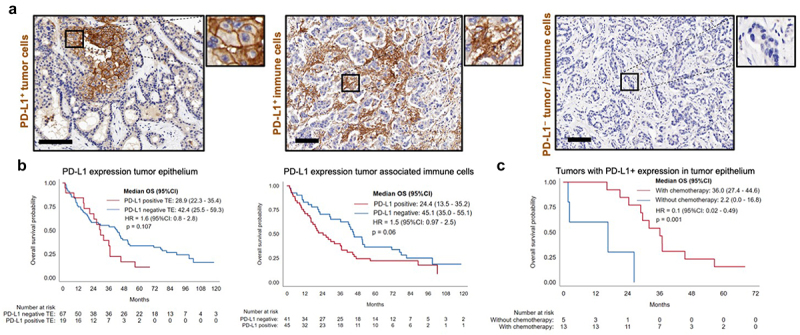
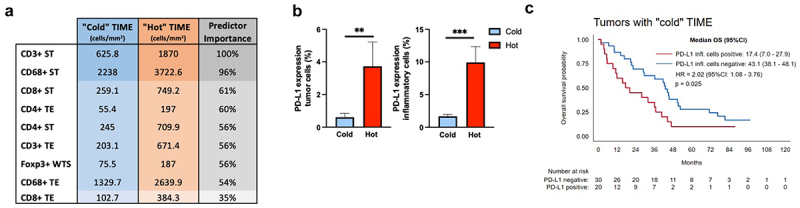
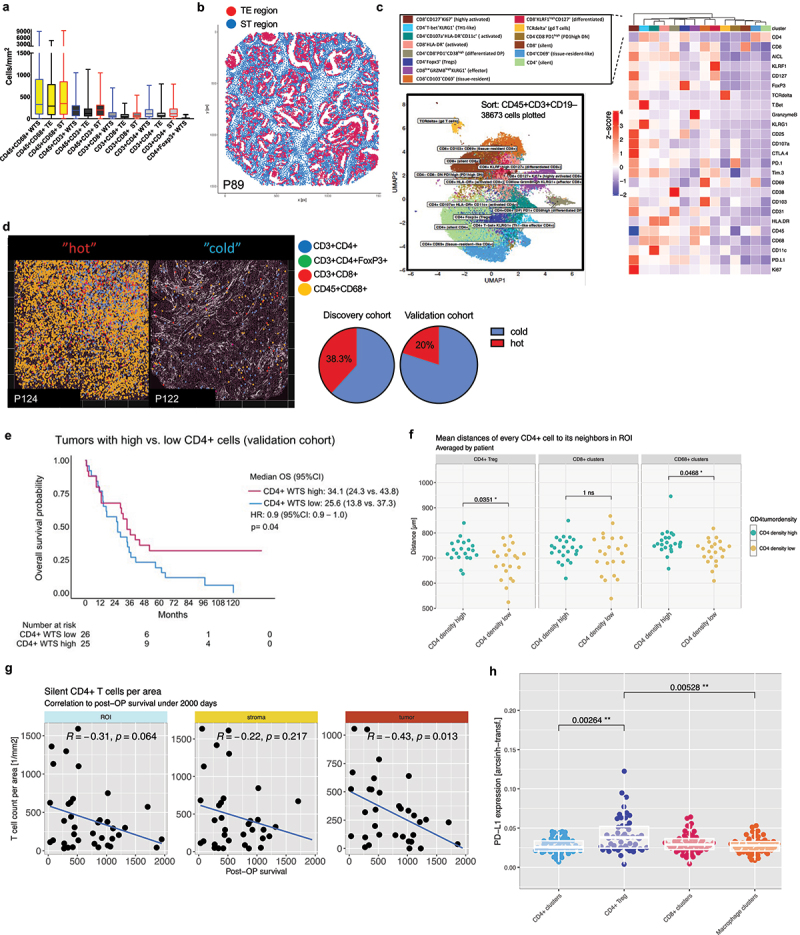
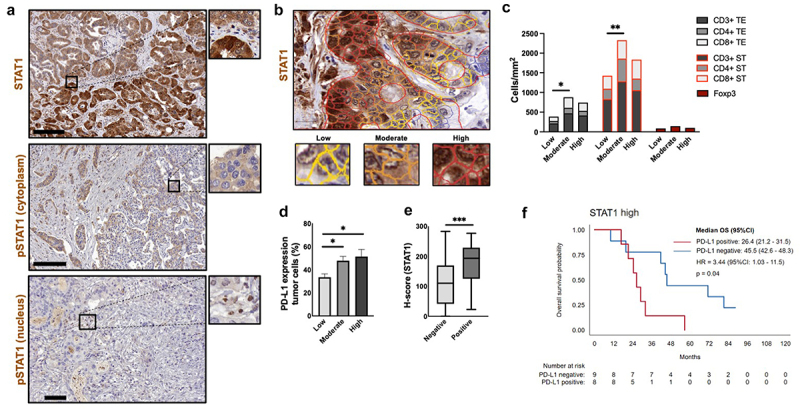
Results: CD68+ cells were the predominant immune cell type in the TIME of ICC. CD4+high T cell density correlated with better overall survival (OS). Prediction modeling together with validation cohort confirmed relevance of CD4+ cells, PD-L1 expression by immune cells in the stroma and N-stage on overall disease outcome. In turn, IMC analyses revealed that silent CD3+CD4+ clusters inversely impacted survival. Among annotated immune cell clusters, PD-L1 was most relevantly expressed by CD4+FoxP3+ cells. A subset of tumors with high density of immune cells ("hot" cluster) correlated with PD-L1 expression and could identify a group of candidates for immune checkpoint inhibition (ICI). Ultimately, higher levels of STAT1 expression were associated with higher lymphocyte infiltration and PD-L1 expression.
Conclusions: These results highlight the importance of CD4+ T cells in immune response against ICC. Secondly, a subset of tumors with "hot" TIME represents potential candidates for ICI, while stimulation of STAT1 pathway could be a potential target to turn "cold" into "hot" TIME in ICC.
Keywords: Immune cell prognosticators; immunomodulation; intrahepatic cholangiocarcinoma; tumor immune microenvironment.
Plain language summary
The tumor immune microenvironment (TIME) plays a critical role in the immune response In many cancers, including intrahepatic cholangiocarcinoma (ICC). Molecular subtyping of the ICC microenvironment already revealed inter-tumoral heterogeneity with variant profiles of immune cell infiltrates. A recent study created an in-depth immune cell atlas of the TIME in biliary tract cancers and could demonstrate the relevance of specific immune cell subpopulations on patient outcome. We are able to provide a distinctive characterization of TIME, separating tumor epithelial- and stroma areas, in a large and representative ICC cohort using digitalized image analysis on tissue microarrays (TMA) as well as multiplex imaging mass cytometry (IMC). The study was designed for identification of immune cell prognosticators allocating institutional ICC patients into a discovery (2008–15) and a validation (2010–19) cohort. Immune cell subpopulations were correlated with clinicopathological characteristics and patient outcome. Our results highlight: i. The important role of CD4+ T cell infiltration in ICC patients; ii. ICC tumors with high density of immune cells associated with PD-L1 expression identifies a subset of patients with variant tumor biology; iii. Stimulation of STAT1 pathway may be a relevant target to turn “cold” into “hot” tumors.
© 2024 The Author(s). Published with license by Taylor & Francis Group, LLC.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Primrose JN, Fox RP, Palmer DH, Malik HZ, Prasad R, Mirza D, Anthony A, Corrie P, Falk S, Finch-Jones M, et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019. 05;20(5):663–673. doi: 10.1016/S1470-2045(18)30915-X. Cited in: Pubmed; PMID 30922733. Epub 20190325. - DOI - PubMed
-
- Strijker M, Belkouz A, van der Geest LG, van Gulik TM, van Hooft JE, de Meijer VE, Haj Mohammad N, de Reuver PR, Verheij J, de Vos-Geelen J, et al. Treatment and survival of resected and unresected distal cholangiocarcinoma: a nationwide study. Acta Oncol. 2019. Jul;58(7):1048–1055. doi: 10.1080/0284186X.2019.1590634. Cited in: Pubmed; PMID 30907207. Epub 20190325. - DOI - PubMed
-
- Oh DY, Lee KH, Lee DW, Yoon J, Kim TY, Bang JH, Nam AR, Oh KS, Kim JM, Lee Y, et al. Gemcitabine and cisplatin plus durvalumab with or without tremelimumab in chemotherapy-naive patients with advanced biliary tract cancer: an open-label, single-centre, phase 2 study. Lancet Gastroenterol Hepatol. 2022. Mar 09;7(6):522–532. eng. Declaration of interests D-YO received research grants from AstraZeneca, Novartis, Array, Eli Lilly, Servier, BeiGene, Merck Sharp & Dohme, and Handok and has been a consultant or adviser for AstraZeneca, Novartis, Genentech, Merck Serono, Bayer, Taiho, ASLAN Pharmaceuticals, Halozyme, Zymeworks, Bristol Myers Squibb, BeiGene, Basilea, and Turning Point. YL, VG, PM, WL, SW, QZ, and MCR are or were employees and shareholders of AstraZeneca. All other authors declare no competing interests Epub 20220309. doi: 10.1016/S2468-1253(22)00043-7. Cited in: Pubmed; PMID 35278356. - DOI - PubMed
-
- Banales JM, Cardinale V, Carpino G, Marzioni M, Andersen JB, Invernizzi P, Lind GE, Folseraas T, Forbes SJ, Fouassier L, et al. Expert consensus document: cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European network for the study of cholangiocarcinoma (ENS-CCA). Nat Rev Gastroenterol Hepatol. 2016. 05;13(5):261–280. doi: 10.1038/nrgastro.2016.51. Cited in: Pubmed; PMID 27095655. Epub 20160420. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous