

FCGR2/3 polymorphisms are associated with susceptibility to Kawasaki disease but do not predict intravenous immunoglobulin resistance and coronary artery aneurysms
- PMID: 39359734
- PMCID: PMC11445592
- DOI: 10.3389/fimmu.2024.1323171
FCGR2/3 polymorphisms are associated with susceptibility to Kawasaki disease but do not predict intravenous immunoglobulin resistance and coronary artery aneurysms
Abstract
Introduction: Kawasaki disease (KD) is a pediatric vasculitis that can result in coronary artery aneurysm (CAA) formation, which is a dangerous complication. Treatment with intravenous immunoglobulin (IVIg) significantly decreases the risk of CAA, possibly through competitive binding to Fc-gamma receptors (FcγRs), which reduces the binding of pathological immune complexes. However, ~20% of children have recrudescence of fever and have an increased risk of CAA. Therefore, we aimed to identify genetic markers at the FCGR2/3 locus associated with susceptibility to KD, IVIg resistance, or CAA.
Materials and methods: We investigated the association of single-nucleotide polymorphisms (SNPs) and copy number variations (CNVs) at the FCGR2/3 locus with KD susceptibility, IVIg resistance, and CAA risk using a family-based test (KD susceptibility) and case-control analyses (IVIg resistance and CAA risk) in different cohorts, adding up to a total of 1,167 KD cases. We performed a meta-analysis on IVIg resistance and CAA risk including all cohorts supplemented by previous studies identified through a systematic search.
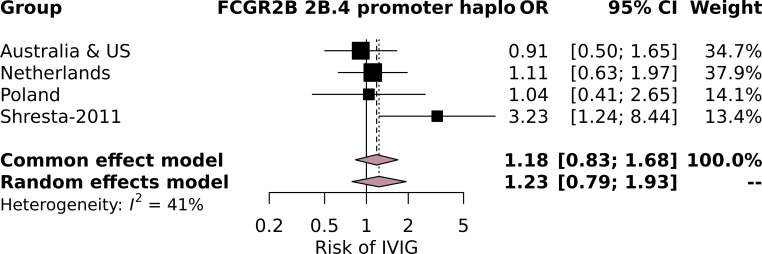
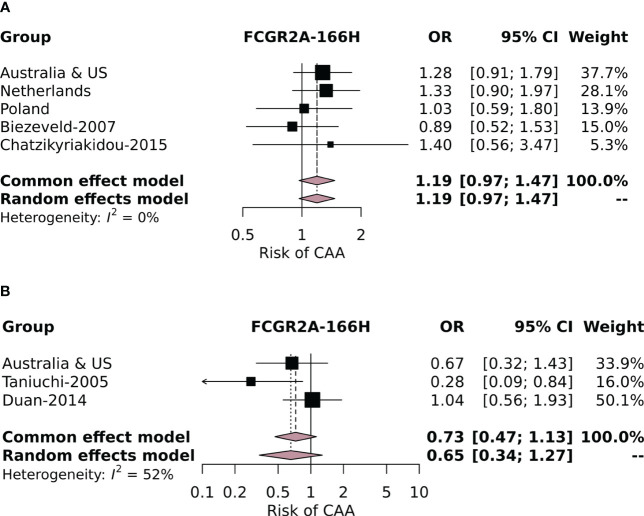
Results: FCGR2A-p.166His was confirmed to be strongly associated with KD susceptibility (Z = 3.17, p = 0.0015). In case-control analyses, all of the investigated genetic variations at the FCGR2/3 locus were generally not associated with IVIg resistance or with CAA risk, apart from a possible association in a Polish cohort for the FCGR3B-NA2 haplotype (OR = 2.15, 95% CI = 1.15-4.01, p = 0.02). Meta-analyses of all available cohorts revealed no significant associations of the FCGR2/3 locus with IVIg resistance or CAA risk.
Discussion: FCGR2/3 polymorphisms are associated with susceptibility to KD but not with IVIg resistance and CAA formation. Currently known genetic variations at the FCGR2/3 locus are not useful in prediction models for IVIg resistance or CAA risk.
Keywords: CAA; FCGR2; FCGR2Ap.His166Arg; FCGR3; IVIg; Kawasaki disease; genetics.
Copyright © 2024 Uittenbogaard, Netea, Tanck, Geissler, Buda, Kowalczyk-Domagała, Okarska-Napierała, van Stijn, Tacke and US Kawasaki Disease Genetics Consortium, Burgner, Shimizu, Burns, Kuipers, Kuijpers and Nagelkerke.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children. Arerugi. (1967) 16:178–222. - PubMed
-
- Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. (2004) 114:1708–33. doi: 10.1542/peds.2004-2182 - DOI - PubMed