

Lung imaging methods: indications, strengths and limitations
- PMID: 39360028
- PMCID: PMC11444493
- DOI: 10.1183/20734735.0127-2023
Lung imaging methods: indications, strengths and limitations
Abstract
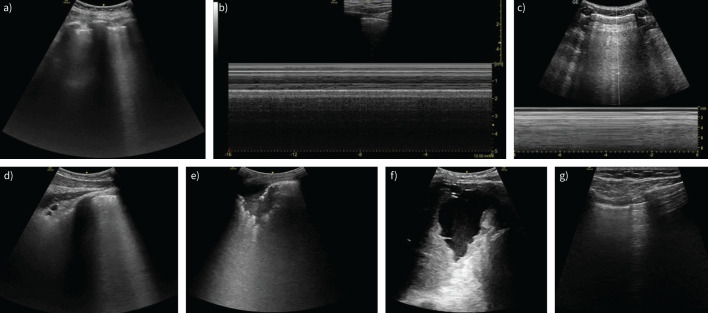
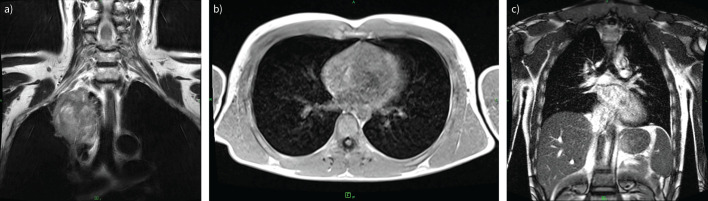
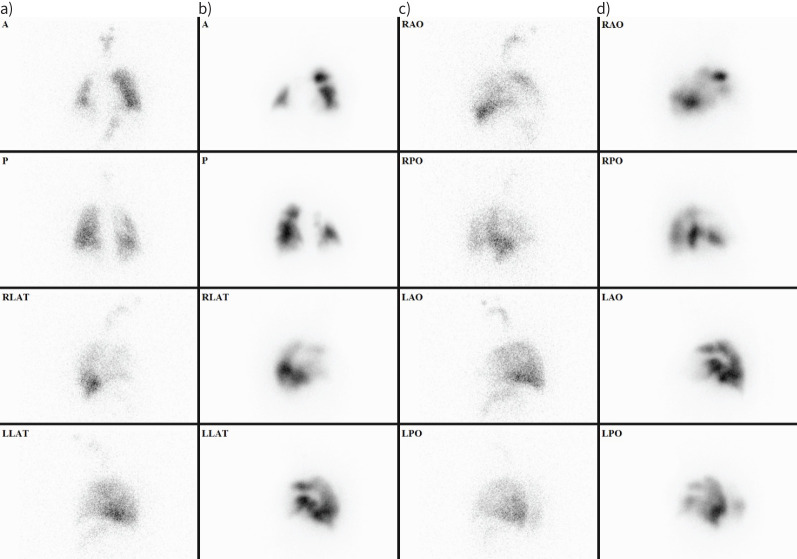
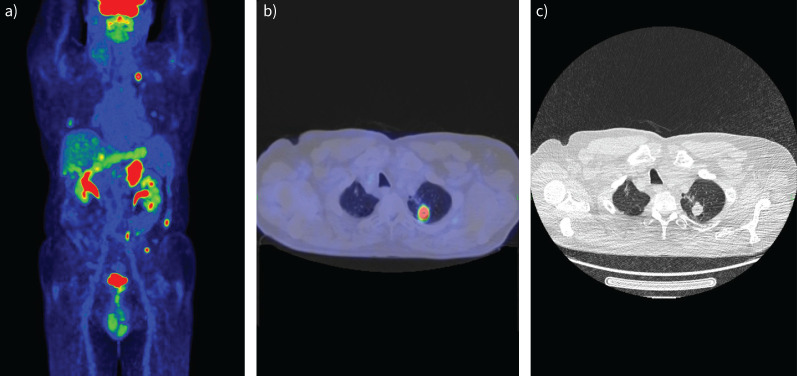
Imaging methods are fundamental tools to detect and diagnose lung diseases, monitor their treatment and detect possible complications. Each modality, starting from classical chest radiographs and computed tomography, as well as the ever more popular and easily available thoracic ultrasound, magnetic resonance imaging and nuclear medicine methods, and new techniques such as photon counting computed tomography, radiomics and application of artificial intelligence, has its strong and weak points, which we should be familiar with to properly choose between the methods and interpret their results. In this review, we present the indications, strengths and main limitations of methods for chest imaging.
Copyright ©ERS 2024.
Conflict of interest statement
Conflict of interest: E.M. Grabczak is a current member of the Breathe editorial board. C.A. Ridge discloses that Cobalt Charity has provided her institution with an education grant to fund a fellow, she is the RSNA Image Wisely co-chair, a ECR Thoracic educational committee member, a European Society of Thoracic Imaging educational committee member and Lung Cancer Journal radiology editor. She is the Director of AI Radiology limited (radiology reporting services). Á.D. Tárnoki is the current chair of the ERS Imaging group. The other authors declare that there is no conflict of interest.
Figures
References
-
- Czibor S, Kiss FJ, Györke T. A fluorodezoxiglükóz pozitron-emissziós tomográfia/komputertomográfia szerepe a tüdőtumorok ellátásában [The role of fluorodeoxyglucose positron emission tomography/computed tomography in the treatment of lung tumours]. Medicina Thoracalis 2021; 74: 319–325.
-
- Radiology Key . Imaging the chest: the chest radiograph. Date last updated: 4 July 2019. Date last accessed: 8 September 2023. https://radiologykey.com/imaging-the-chest-the-chest-radiograph/
-
- Kári B, Karlinger K, Légrády D, et al., eds. Medical Imaging. Budapest, Semmelweis University and Budapest University of Technology and Economics, 2019. http://oftankonyv.reak.bme.hu/tiki-index.php?page=Orvosi_Posztgradu%C3%A...
Publication types
LinkOut - more resources
Full Text Sources