

Treatment Challenges and Controversies in the Management of Critically Ill Diabetic Ketoacidosis (DKA) Patients in Intensive Care Units
- PMID: 39360087
- PMCID: PMC11446492
- DOI: 10.7759/cureus.68785
Treatment Challenges and Controversies in the Management of Critically Ill Diabetic Ketoacidosis (DKA) Patients in Intensive Care Units
Abstract
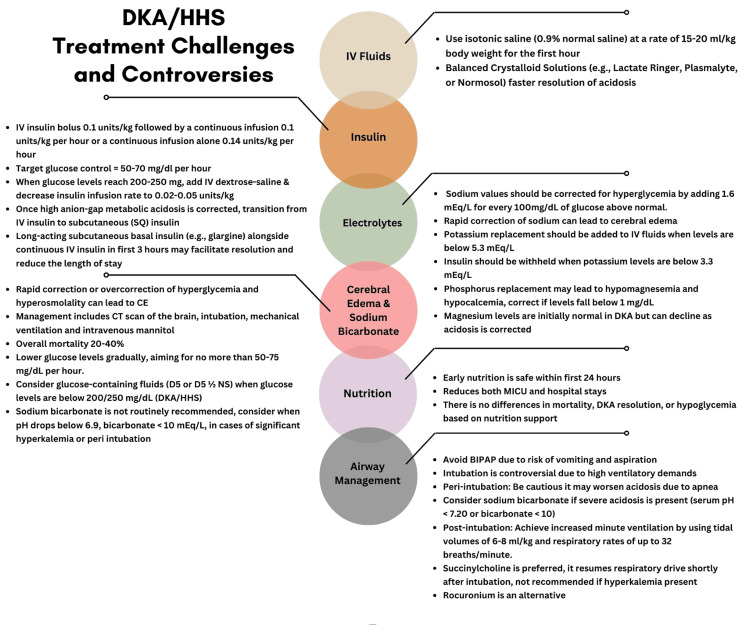
This review discusses the challenges and controversies in the treatment of diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS). Key areas include the selection of intravenous (IV) fluids, insulin therapy, strategies for preventing and monitoring cerebral edema (CE) by managing hyperglycemia overcorrection, electrolyte replacement, timing of nutrition, use of IV sodium bicarbonate, and airway management in critically ill DKA patients. Isotonic normal saline remains the standard for initial fluid resuscitation, though balanced solutions have been shown to have faster DKA resolution. Current guidelines recommend using continuous IV insulin for DKA management after fluid status has been restored potassium levels have been achieved and subcutaneous (SQ) insulin is started only after the resolution of metabolic acidosis. In comparison, the British guidelines recommend using SQ insulin glargine along with continuous regular IV insulin, which has shown faster DKA resolution and shorter hospital stays compared to continuous IV insulin alone. Although rare, rapid overcorrection of hyperglycemia with fluids and insulin can lead to CE, seizures, and death. Clinicians should be aware of risk factors and preventive strategies for CE. DKA frequently involves multiple electrolyte abnormalities, such as hypokalemia, hypophosphatemia, and hypomagnesemia and regular monitoring is essential for DKA management. Early initiation of oral nutrition has been shown to reduce intensive care unit and overall hospital length of stay. For impending respiratory failure, Bilevel positive airway pressure is not recommended due to aspiration risks. Instead, intubation and mechanical ventilation, with monitoring and management of acid-base and fluid status, are recommended. The use of sodium bicarbonate is discouraged due to the potential for worsening ketosis, hypokalemia, and risk of CE. However, IV sodium bicarbonate can be considered if the serum pH falls below 6.9, or when serum pH is less than 7.2 and/or serum bicarbonate levels are below 10 mEq/L, pre-and post-intubation, to prevent metabolic acidosis and hemodynamic collapse that occurs from apnea during intubation. Managing DKA and HHS in critically ill patients includes using balanced IV fluid solutions to restore volume status, followed by continuous IV insulin, early use of SQ glargine insulin, electrolyte replacement, and monitoring, CE preventive strategies by avoiding hyperglycemia overcorrection, early nutritional support, and appropriate airway management.
Keywords: cerebral edema and airway management; diabetic ketoacidosis (dka); electrolyte management; hyperosmolar hyperglycemic state (hhs); insulin therapy; intravenous fluids; nutritional support.
Copyright © 2024, Dunn et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Management of hyperglycemic crises in patients with diabetes. Kitabchi AE, Umpierrez GE, Murphy MB, Barrett EJ, Kreisberg RA, Malone JI, Wall BM. Diabetes Care. 2001;24:131–153. - PubMed
-
- Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Crit Care Med. 2007;35:1244–1250. - PubMed
-
- An update on the incidence and burden of diabetic ketoacidosis in the U.S. Ramphul K, Joynauth J. Diabetes Care. 2020;43:0–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources