

Laparoscopic versus open repair for peptic ulcer perforation: a systematic review, meta-analysis and trial sequential analysis of randomised controlled trials. Time to conclude!
- PMID: 39361132
- PMCID: PMC12043367
- DOI: 10.1308/rcsann.2024.0082
Laparoscopic versus open repair for peptic ulcer perforation: a systematic review, meta-analysis and trial sequential analysis of randomised controlled trials. Time to conclude!
Abstract
Introduction: The aim of this study was to investigate comparative outcomes of laparoscopic and open repair for peptic ulcer perforation (PUP).
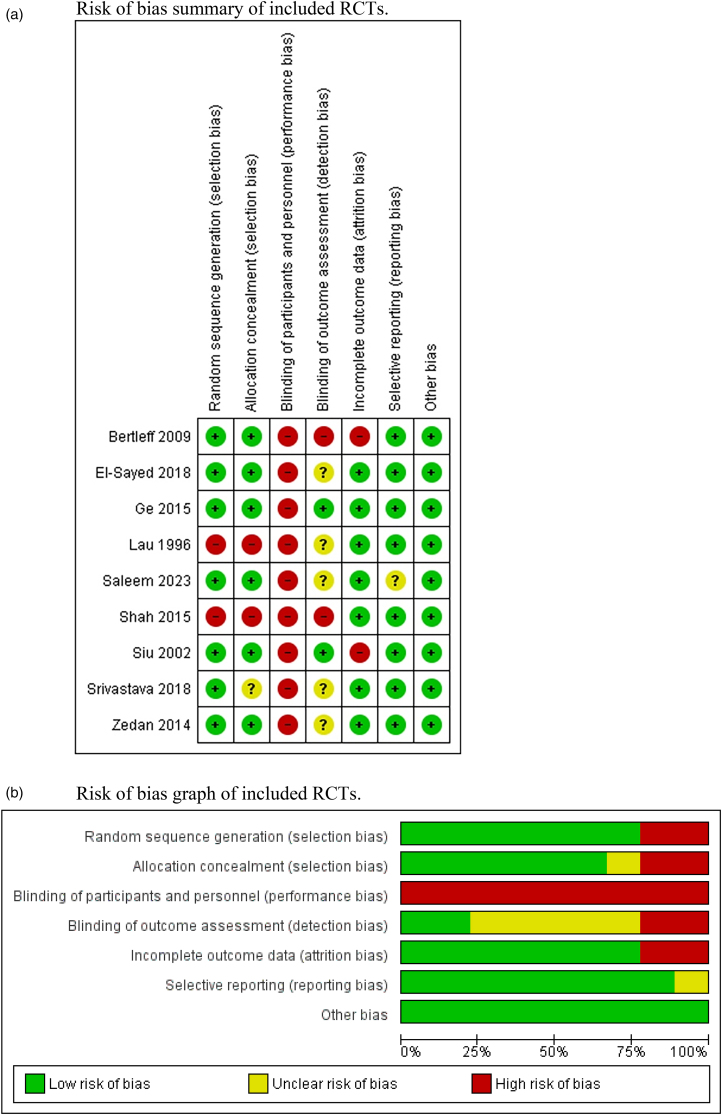
Methods: A PRISMA-compliant systematic review with a PROSPERO-registered protocol (registration number CRD42024529286) was conducted. All randomised controlled trials (RCTs) involving PUP patients managed by laparoscopic or open repair were identified and their risk of bias assessed. Outcome syntheses for perioperative mortality and morbidities, need for reoperation, procedure time and length of hospital stay were conducted using random-effects modelling to calculate risk ratios (RR) or mean difference (MD) with 95% confidence intervals (CI).
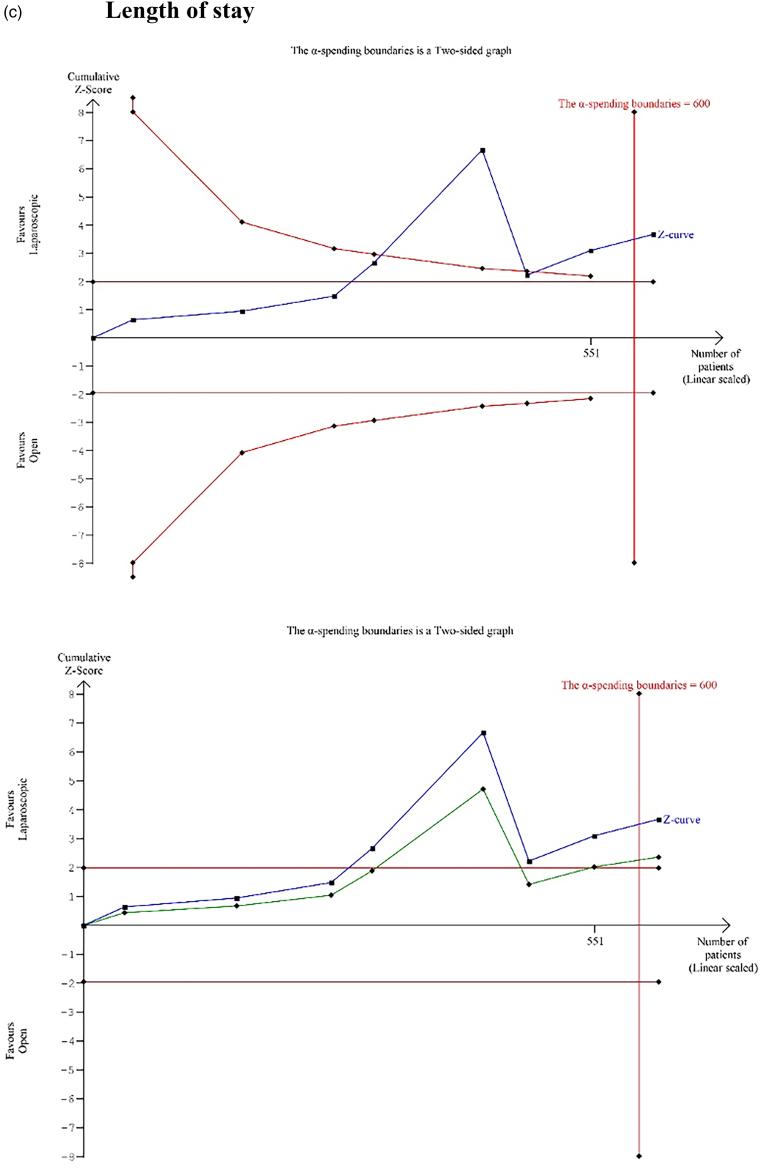
Findings: Nine RCTs met the inclusion criteria, enrolling 670 patients of whom 317 were randomised to receive laparoscopic surgery and 353 were managed with open surgery. Laparoscopic repair of PUP significantly reduced mortality (RR 0.37, p = 0.03), total complications (RR 0.57, p = 0.0009), ileus (RR 0.43, p = 0.04), wound complications (RR 0.36, p < 0.0001) and length of hospital stay (MD -2.37, p = 0.0003) compared with the open approach. There were no significant differences in rate of postoperative leak (RR 2.00, 95% CI 0.74-5.41, p = 0.17), abdominal collection (RR 1.19, 95% CI 0.46-3.07, p = 0.72), sepsis (RR 1.17, 95% CI 0.39-3.52, p = 0.65), respiratory complications (RR 0.68, 95% CI 0.32-1.46, p = 0.32), reoperation (RR 1.74, 95% CI 0.57-5.30, p = 0.33) and operating time (MD 15.31, 95% CI -4.86 to 35.47, p = 0.14) between the two groups.
Conclusions: Laparoscopic repair of PUP is associated with significantly lower mortality and morbidity and shorter length of stay compared with the open approach. The laparoscopic approach should be the management of choice subject to the existence of laparoscopic expertise.
Keywords: Meta-analysis; Outcomes; Peptic ulcer disease; Surgery.
Figures







References
-
- Ocasio Quinones GA, Woolf A. Duodenal ulcer. In: StatPearls. Treasure Island: (FL: ): StatPearls Publishing. Copyright © 2023. StatPearls Publishing LLC; 2023.
-
- Bordin DS, Shengelia MI, Ivanova VA, Voynovan IN. The history of the discovery of the Helicobacter pylori. Ter Arkh 2022; 94: 283–288. - PubMed
-
- Ansari D, Torén W, Lindberg Set al. . Diagnosis and management of duodenal perforations: a narrative review. Scand J Gastroenterol 2019; 54: 939–944. - PubMed
-
- Amini A, Lopez RA. Duodenal perforation. In: StatPearls. Treasure Island: (FL: ): StatPearls Publishing. Copyright © 2023, StatPearls Publishing LLC; 2023. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous