

Time to COVID-19 Vaccination by Language and Country of Origin
- PMID: 39361282
- PMCID: PMC11450518
- DOI: 10.1001/jamanetworkopen.2024.37388
Time to COVID-19 Vaccination by Language and Country of Origin
Abstract
Importance: Disparities in COVID-19 vaccination rates by race and ethnicity are well documented. Less is known about primary language and COVID-19 vaccine uptake.
Objective: To describe the time to COVID-19 primary series vaccination and booster doses by primary language and country of origin.
Design, setting, and participants: This retrospective cohort study included patients aged 6 months or older with at least 1 health encounter from July 1, 2019, to June 30, 2023, at a single health care system serving patients across Minnesota and western Wisconsin.
Exposure: Primary language and country of origin documented in the electronic health record.
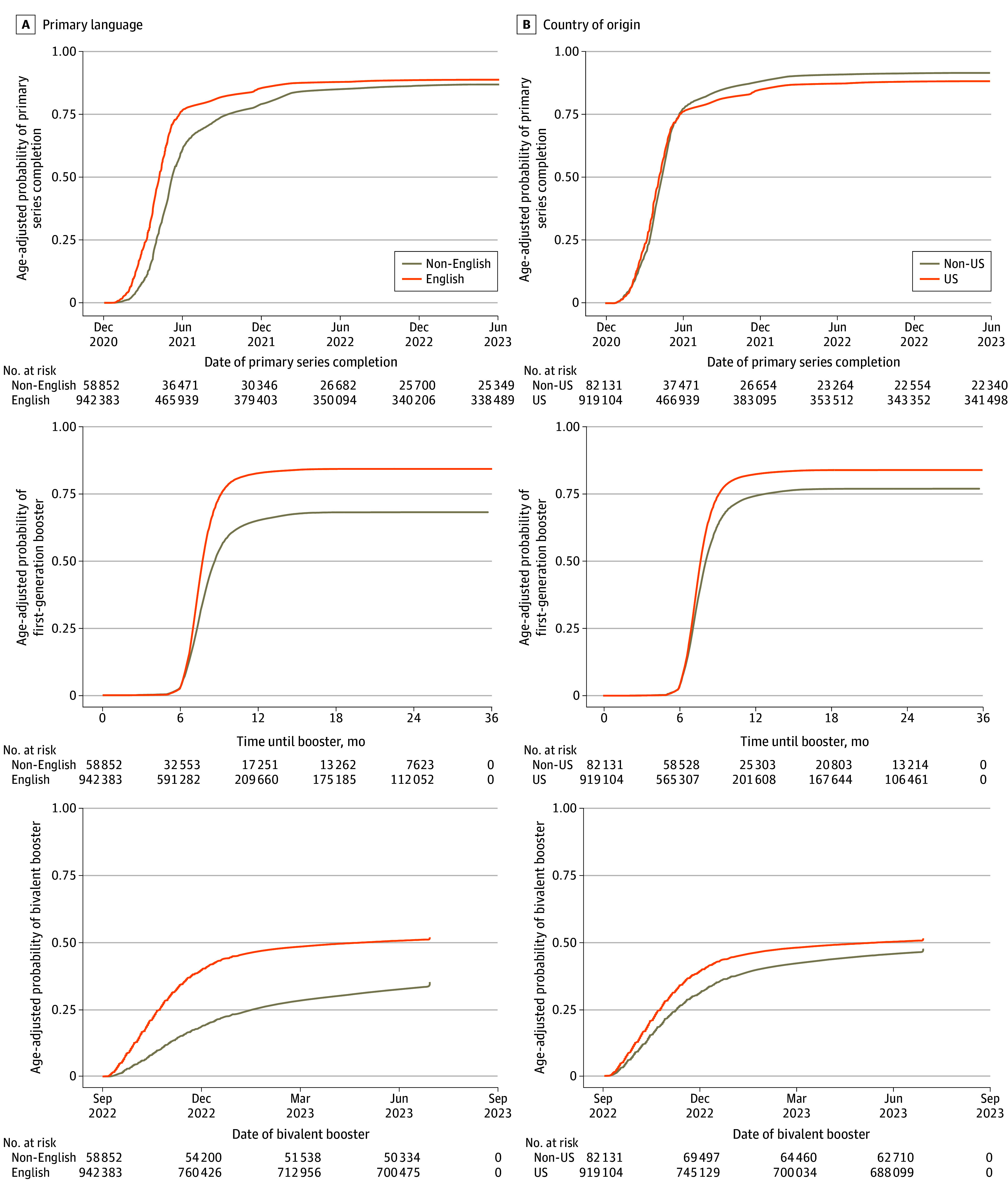
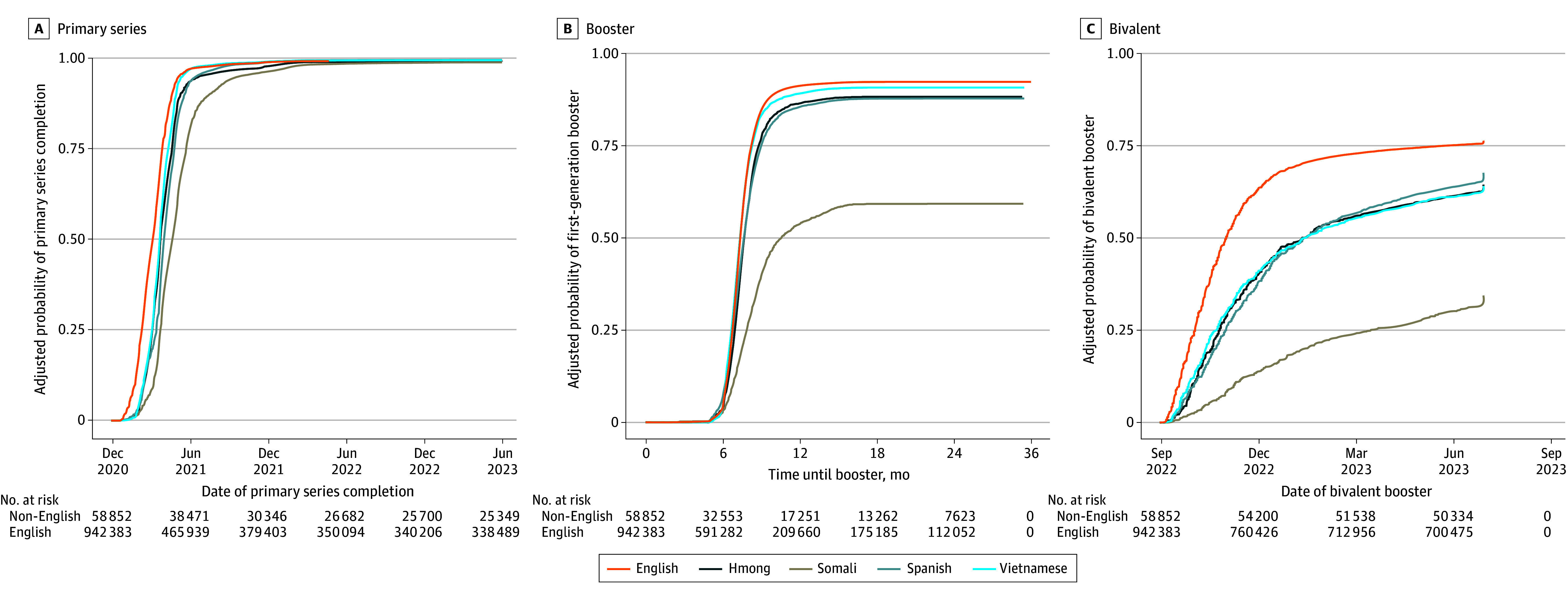
Main outcomes and measures: Three COVID-19 vaccine coverage outcomes were evaluated: (1) primary series (1 Ad26.COV.S vaccine or 2 mRNA COVID-19 vaccines), (2) first-generation booster (primary series Ad26.COV.S vaccine plus 1 Ad26.COV.S or mRNA COVID-19 vaccine at least 2 months after the second dose or primary series mRNA vaccine plus 1 mRNA vaccine at least 5 months after the second dose), and (3) bivalent booster. Vaccine coverage was described by patient characteristics. Associations of primary language, race and ethnicity, and other patient characteristics with COVID-19 vaccine uptake were evaluated using time-to-event analysis in multivariable Cox proportional hazards regression models, and adjusted hazard ratios (AHRs) with 95% CIs were reported.
Results: There were 1 001 235 patients included (53.7% female). Most patients reported English as a primary language (94.1%) and were born in the US (91.8%). Primary series coverage was 63.7%; first-generation booster coverage, 64.4%; and bivalent booster coverage, 39.5%. Coverage for all outcomes was lower among those with a non-English primary language compared with English as the primary language (56.9% vs 64.1% for primary series; 47.5% vs 65.3% for first-generation booster; 26.2% vs 40.3% for bivalent booster). Those with a non-English primary language had lower COVID-19 vaccine uptake for the primary series (AHR, 0.85; 95% CI, 0.84-0.86), first-generation booster (AHR, 0.74; 95% CI, 0.73-0.75), and bivalent booster (AHR, 0.65; 95% CI, 0.64-0.67) compared with patients with English as their primary language. Non-US-born patients had higher primary series uptake compared with US-born patients (AHR, 1.19; 95% CI, 1.18-1.20) but similar first-generation booster (AHR, 1.01; 95% CI, 0.99-1.02) and bivalent booster (AHR, 1.00; 95% CI, 0.98-1.02) uptake.
Conclusions and relevance: In this retrospective cohort study, patients with a non-English primary language had both lower coverage and delays in receiving COVID-19 vaccines compared with those with English as their primary language. Reporting on language may identify health disparities that can be addressed with language-specific interventions.
Conflict of interest statement
Figures
References
-
- Nguyen KH, Anneser E, Toppo A, Allen JD, Scott Parott J, Corlin L. Disparities in national and state estimates of COVID-19 vaccination receipt and intent to vaccinate by race/ethnicity, income, and age group among adults ≥ 18 years, United States. Vaccine. 2022;40(1):107-113. doi: 10.1016/j.vaccine.2021.11.040 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
