

USPSTF Colorectal Cancer Screening Recommendation and Uptake for Individuals Aged 45 to 49 Years
- PMID: 39361285
- PMCID: PMC11450516
- DOI: 10.1001/jamanetworkopen.2024.36358
USPSTF Colorectal Cancer Screening Recommendation and Uptake for Individuals Aged 45 to 49 Years
Abstract
Importance: In May 2021, the US Preventive Services Task Force (USPSTF) issued a grade B recommendation encouraging colorectal cancer (CRC) screening among average-risk individuals aged 45 to 49 years. The patterns of screening uptake and possible socioeconomic disparities in screening in this age group remain unknown.
Objective: To evaluate changes in CRC screening uptake among average-risk individuals aged 45 to 49 years after the USPSTF recommendation was issued in 2021.
Design, setting, and participants: This retrospective cohort study used deidentified claims data from commercially insured Blue Cross Blue Shield beneficiaries aged 45 to 49 years across the US between January 1, 2017, and December 31, 2022.
Exposure: Publication of the May 2021 USPSTF CRC screening recommendation for adults aged 45 to 49 years.
Main outcomes and measures: Absolute and relative changes in screening uptake were compared between a 20-month period preceding (May 1, 2018, to December 31, 2019) and a 20-month period following (May 1, 2021, to December, 31, 2022) the USPSTF recommendation. Interrupted time-series analysis and autoregressive integrated moving average models were used to evaluate changes in screening rates, adjusting for temporal autocorrelation and seasonality.
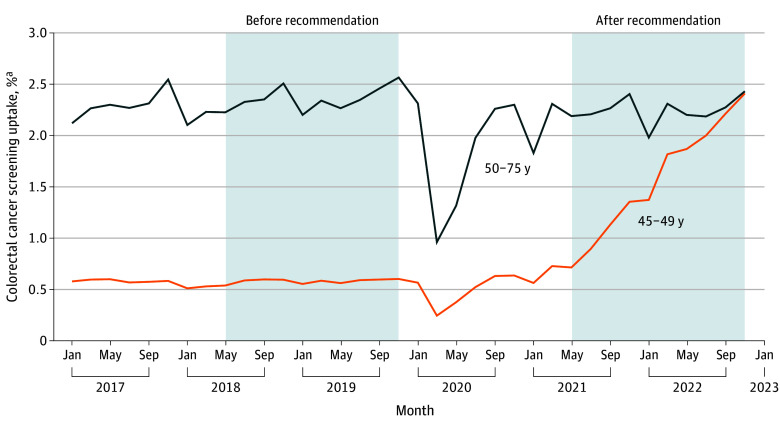
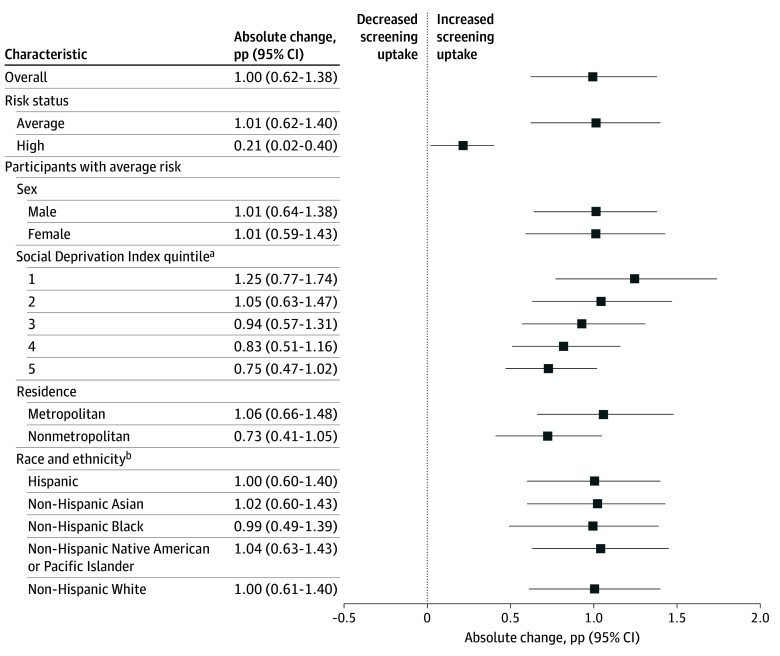
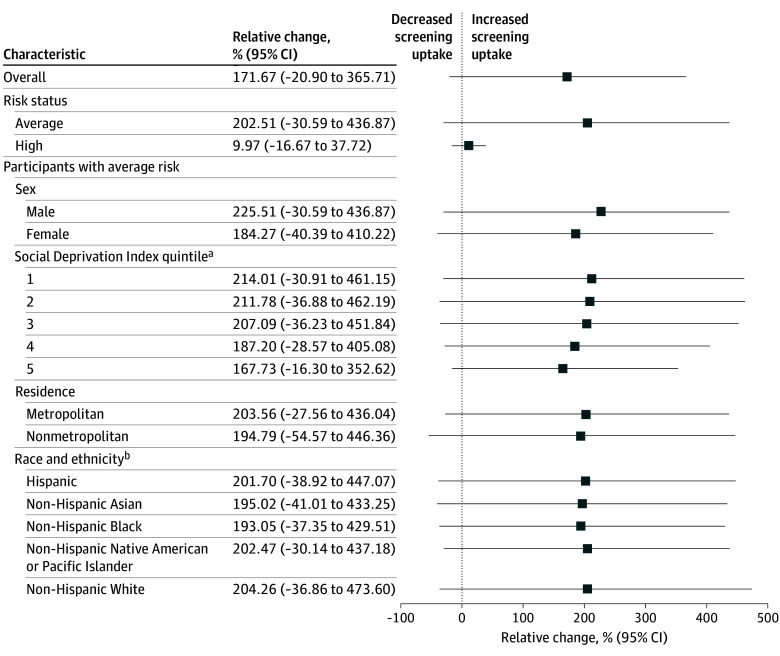
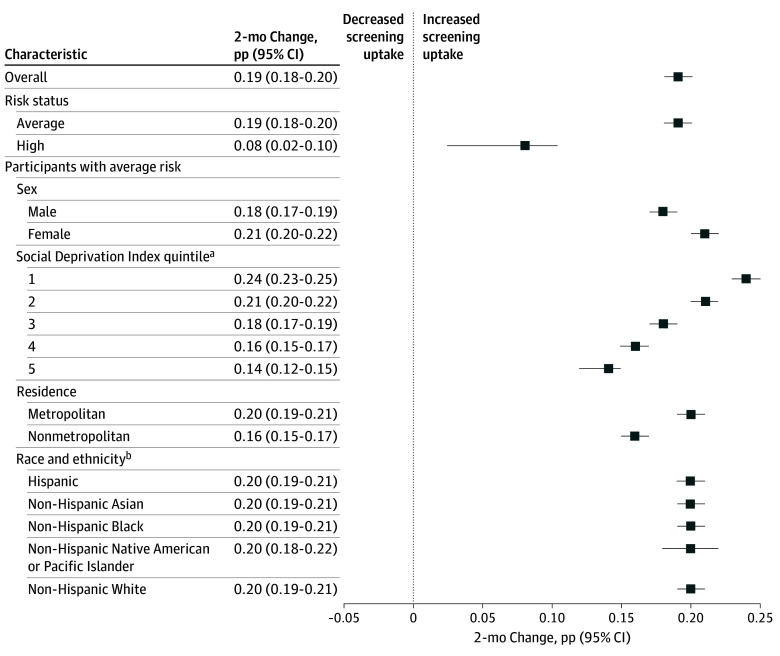
Results: In this cohort study of 10 221 114 distinct beneficiaries aged 45 to 49 years (mean [SD] age, 47.04 [1.41] years; 51.04% female), bimonthly mean (SD) numbers of average-risk beneficiaries were 3 213 935 (31 508) and 2 923 327 (105 716) in the prerecommendation and postrecommendation periods, respectively. Mean (SD) screening uptake increased from 0.50% (0.02%) to 1.51% (0.59%) between the 2 periods (P < .001), representing an absolute change of 1.01 percentage points (95% CI, 0.62-1.40 percentage points) but no significant relative change (202.51%; 95% CI, -30.59% to 436.87%). Compared with average-risk beneficiaries residing in areas with the lowest socioeconomic status (SES), those residing in areas with the highest SES experienced the largest absolute change in screening (1.25 [95% CI, 0.77-1.74] percentage points vs 0.75 [95% CI, 0.47-1.02] percentage points), but relative changes were not significant (214.01% [95% CI, -30.91% to 461.15%] vs 167.73% [95% CI, -16.30% to 352.62%]). After the recommendation was issued, the screening uptake rate also increased fastest among average-risk beneficiaries residing in the areas with highest SES (0.24 [95% CI, 0.23-0.25] percentage points every 2 months) and metropolitan areas (0.20 [95% CI, 0.19-0.21] percentage points every 2 months).
Conclusions and relevance: This study found that among privately insured beneficiaries aged 45 to 49 years, CRC screening uptake increased after the USPSTF recommendation, with potential disparities based on SES and locality.
Conflict of interest statement
Figures
Comment in
-
USPSTF Recommendations and Colorectal Cancer in Younger Adults-Current Challenges and Future Opportunities.JAMA Netw Open. 2024 Oct 1;7(10):e2436305. doi: 10.1001/jamanetworkopen.2024.36305. JAMA Netw Open. 2024. PMID: 39361287 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
