

Real-world impact of emicizumab and immunosuppression on acquired hemophilia A: a multicenter US cohort
- PMID: 39361769
- PMCID: PMC11612364
- DOI: 10.1182/bloodadvances.2024013882
Real-world impact of emicizumab and immunosuppression on acquired hemophilia A: a multicenter US cohort
Abstract
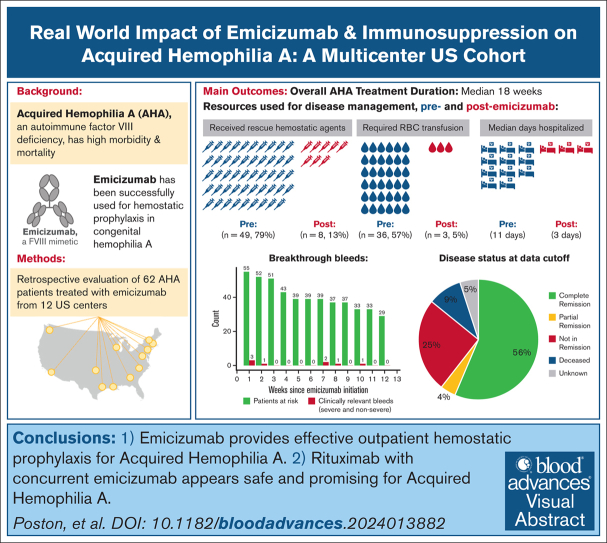
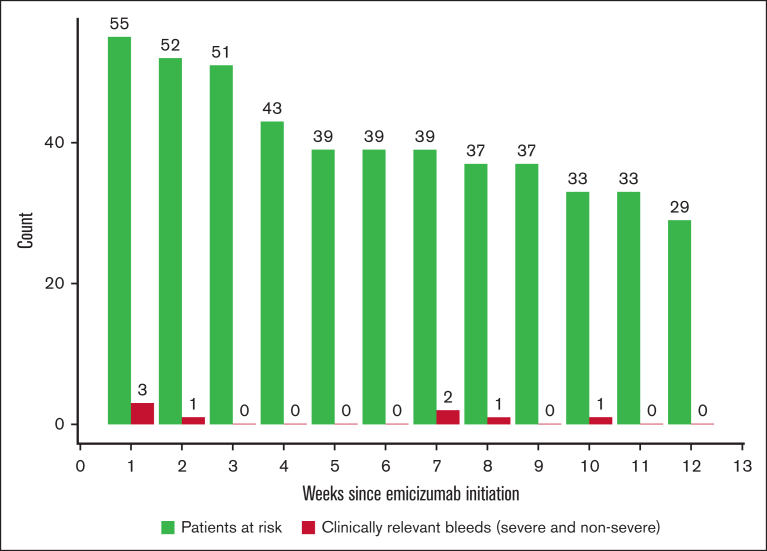
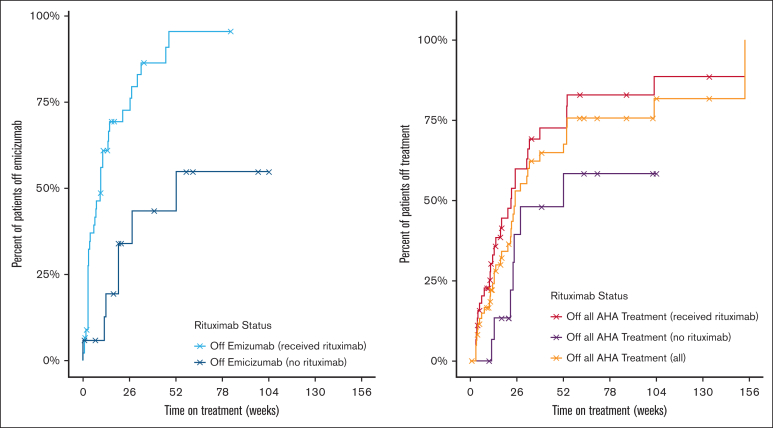
Acquired hemophilia A (AHA) is an autoimmune bleeding disorder that is caused by factor VIII (FVIII) autoantibodies with high morbidity and mortality due to bleeding and complications from immunosuppression (IST). To address the real-world implications of the FVIII mimetic antibody, emicizumab, and the role of IST, we retrospectively collected de-identified data on 62 patients with AHA who were treated off-label with emicizumab for a median of 10 weeks at 12 US-based hemophilia treatment centers. Most patients (95.2%) had acute bleeding at diagnosis, and 62.9% had partial or no control of bleeds despite the use of hemostatic agents at the time emicizumab was started. The main reason for initiating emicizumab was outpatient bleeding prophylaxis. After initiation of emicizumab, 87.1% had no additional bleeds. There were 6 breakthrough bleeds (2 spontaneous) in 5 patients and no fatal bleeding events during maintenance emicizumab treatment. The mean breakthrough bleed rate per patient-week was 0.02 (95% confidence interval, 0.0-0.03) during the first 12 weeks of emicizumab for the 55 patients with at least 12 weeks of follow-up. Of these patients, 92.7% received IST and 74.5% were prescribed rituximab-based regimens. Complete resolution of inhibitor and normalization of FVIII levels occurred in 56% overall and in 63% of the patients treated with rituximab. Overall, the median time to discontinuation of emicizumab and IST was 18 weeks. Two patients had thrombotic events while on emicizumab, but no adverse events were attributed to emicizumab and there were no infections attributed to IST. Emicizumab provides effective outpatient bleeding prophylaxis for AHA, and concurrent IST may further mitigate bleeding.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.v.D. reports receiving honoraria for participating in scientific advisory board panels, consultations, and speaking engagements for BioMarin, Regeneron, Pfizer, Bioverativ/Sanofi, CSL Behring, Novo Nordisk, Precision Medicine, SparX Therapeutics, Takeda, Genentech, and uniQure, and is a cofounder and member of the board of directors of Hematherix LLC, a biotech company that is developing superFVa therapy for bleeding complications. A.P. reports receiving research support from Shire/Takeda, Genentech/Hoffman LaRoche; serving on advisory boards for Genentech, Shire/Takeda, Sigilon, and uniQure; and serving as a consultant for Aspa, I-Mab, and Sunovion. C.M.K. reports receiving research support from Bayer, Genentech, Novo Nordisk, Octapharma, and Regeneron; serving on advisory boards for Bayer, Genentech, Novo Nordisk, Octapharma, Pfizer, and Takeda; and serving on data and safety monitoring boards for Bayer and Octapharma. C.W. reports serving as a consultant for Genentech, Novo Nordisk, CSL Behring, BioMarin, and Sanofi. E.C.C. reports serving as a consultant for Guidepoint, Sentiment, Enos Health, Lumanity, and AbbVie. J.N.P. reports serving as a consultant for TeraImmune. J.Y.Z. reports serving as a consultant for Diagonal Therapeutics. L.M.M. reports serving as a consultant for Sanofi, Sobi, CSL Behring, Spark, BioMarin, Novo Nordisk, Takeda, and Pfizer; receiving research funding from Sanofi; and serving on speakers' bureaus for Sanofi and CSL Behring. M.A.E. reports serving as a consultant for Genentech/Roche, Novo Nordisk, CSL Behring, Takeda, Sanofi, Bayer, HEMA Biologics, LFB, Regeneron, BioMarin, and the National Bleeding Disorders Foundation. M.J. reports serving as a consultant for and receiving research funding from Genentech and serving as a consultant for Takeda, Sanofi, Bioamarin, CSL Behring, and Octapharma. O.K. reports serving as a consultant for BioMarin, Sanofi, Pfizer, Genentech, Kedrion, Bayer, and Novo Nordisk. P.E. reports serving as a consultant for Genentech. R.K.-J. reports receiving research support from Genentech, Sanofi, and Pfizer, and serving on advisory boards and as a consultant for Roche/Genentech and Regeneron. The remaining authors declare no competing financial interests.
Figures
References
-
- Knoebl P, Marco P, Baudo F, et al. Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH2) J Thromb Haemost. 2012;10(4):622–631. - PubMed
-
- Tengborn L, Baudo F, Huth-Kühne A, et al. Pregnancy-associated acquired haemophilia A: results from the European Acquired Haemophilia (EACH2) registry. BJOG. 2012;119(12):1529–1537. - PubMed
-
- Borg JY, Guillet B, Le Cam-Duchez V, Goudemand J, Lévesque H, SACHA Study Group Outcome of acquired haemophilia in France: the prospective SACHA (Surveillance des Auto antiCorps au cours de l’Hémophilie Acquise) registry. Haemophilia. 2013;19(4):564–570. - PubMed
-
- Kruse-Jarres R, St-Louis J, Greist A, et al. Efficacy and safety of OBI -1, an antihaemophilic factor VIII (recombinant), porcine sequence, in subjects with acquired haemophilia A. Haemophilia. 2015;21(2):162–170. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
