Fungal lung disease
- PMID: 39362667
- PMCID: PMC11602666
- DOI: 10.1183/13993003.00803-2024
Fungal lung disease
Abstract
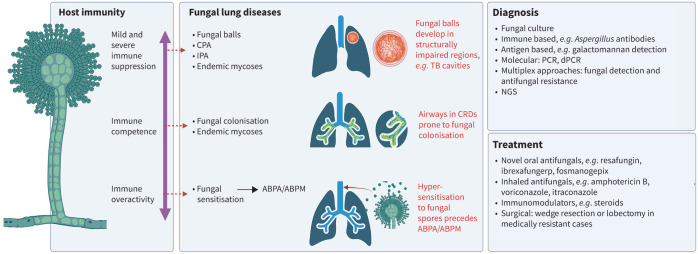
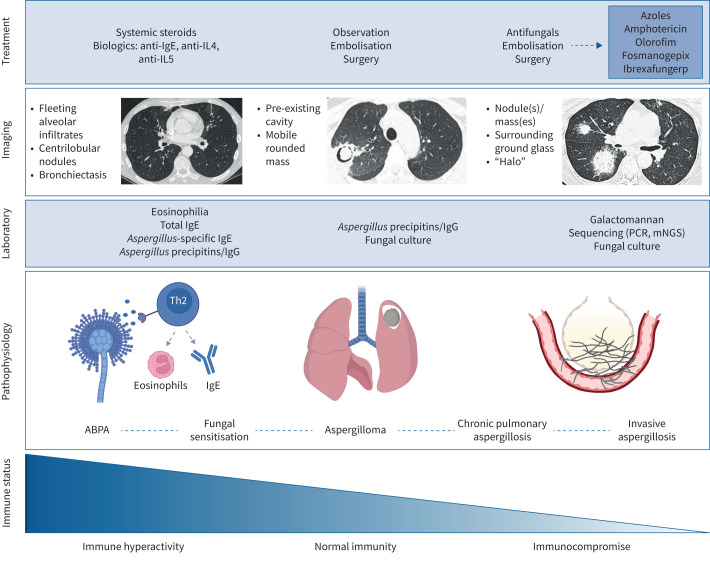
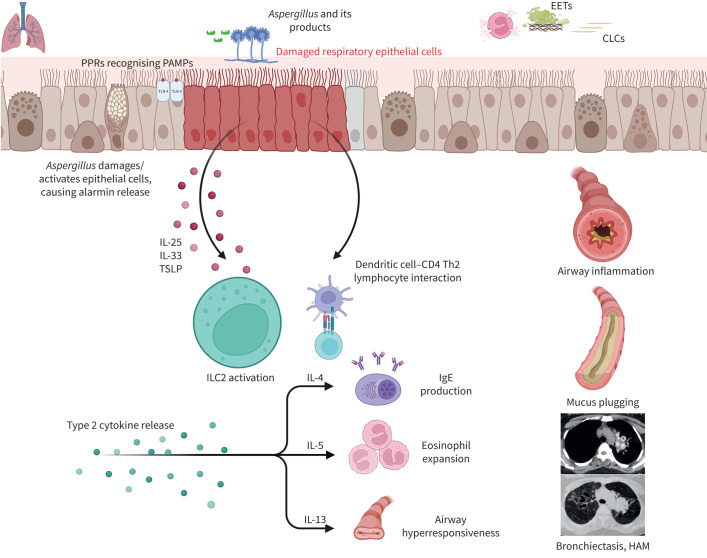
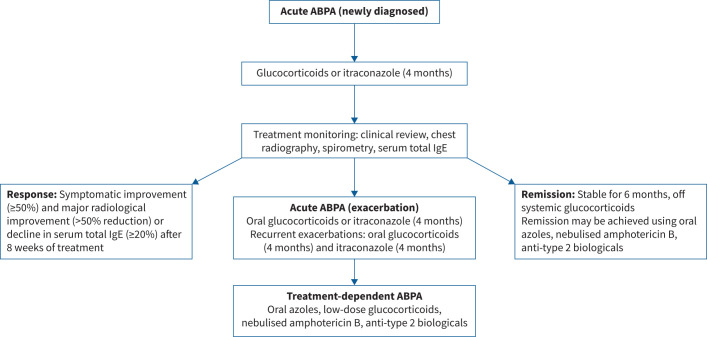
Fungal lung disease encompasses a wide spectrum of organisms and associated clinical conditions, presenting a significant global health challenge. The type and severity of disease are determined by underlying host immunity and infecting fungal strain. The most common group of diseases are associated with the filamentous fungus Aspergillus species and include allergic bronchopulmonary aspergillosis, sensitisation, aspergilloma and chronic and invasive pulmonary aspergillosis. Fungal lung disease remains epidemiologically heterogenous and is influenced by geography, environment and host comorbidities. Diagnostic modalities continue to evolve and now include novel molecular assays and biomarkers; however, persisting challenges include achieving rapid and accurate diagnosis, particularly in resource-limited settings, and in differentiating fungal infection from other pulmonary conditions. Treatment strategies for fungal lung diseases rely mainly on antifungal agents but the emergence of drug-resistant strains poses a substantial global threat and adds complexity to existing therapeutic challenges. Emerging antifungal agents and increasing insight into the lung mycobiome may offer fresh and personalised approaches to diagnosis and treatment. Innovative methodologies are required to mitigate drug resistance and the adverse effects of treatment. This state-of-the-art review describes the current landscape of fungal lung disease, highlighting key clinical insights, current challenges and emerging approaches for its diagnosis and treatment.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: S.H. Chotirmall has served on advisory boards for CSL Behring, Pneumagen Ltd and Boehringer Ingelheim, on data safety monitoring boards for Inovio Pharmaceuticals and Imam Abdulrahman Bin Faisal University, and has received personal fees from AstraZeneca and Chiesi Farmaceutici, all unrelated to this work. The remaining authors have no potential conflicts of interest to disclose.
Figures