

FGF21 modulates immunometabolic homeostasis via the ALOX15/15-HETE axis in early liver graft injury
- PMID: 39362839
- PMCID: PMC11449914
- DOI: 10.1038/s41467-024-52379-2
FGF21 modulates immunometabolic homeostasis via the ALOX15/15-HETE axis in early liver graft injury
Abstract
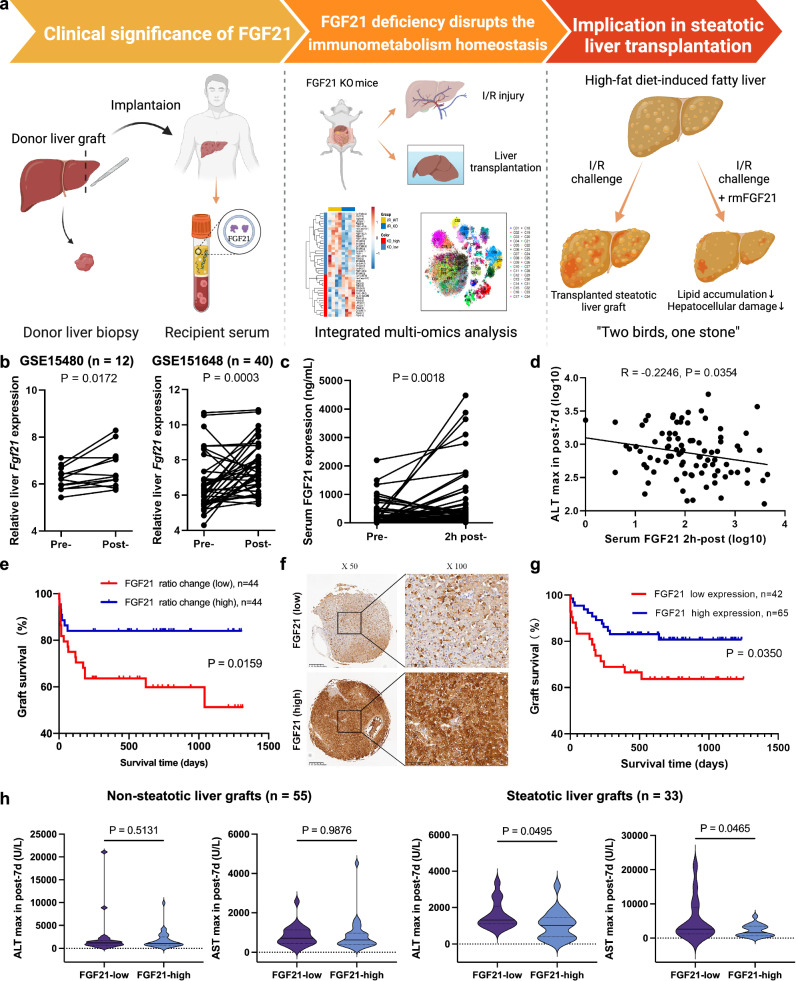
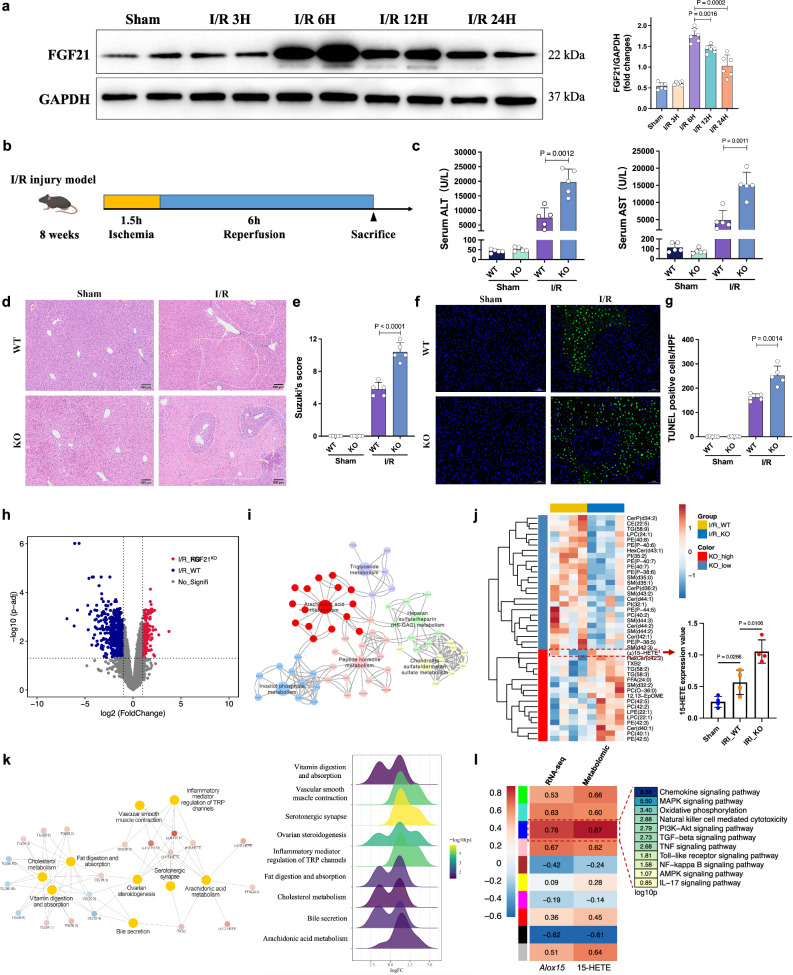
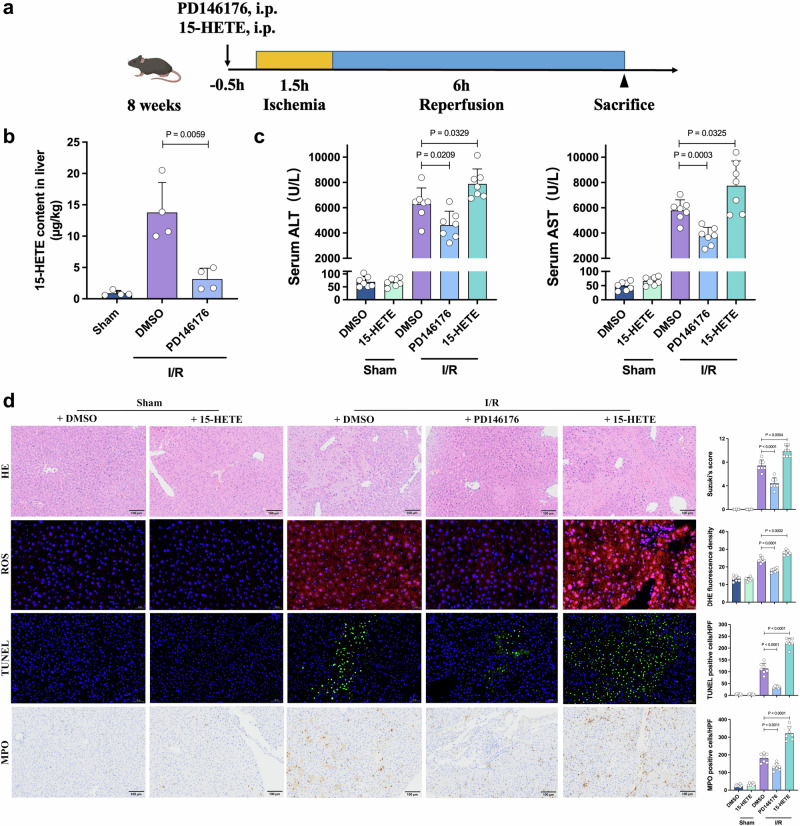
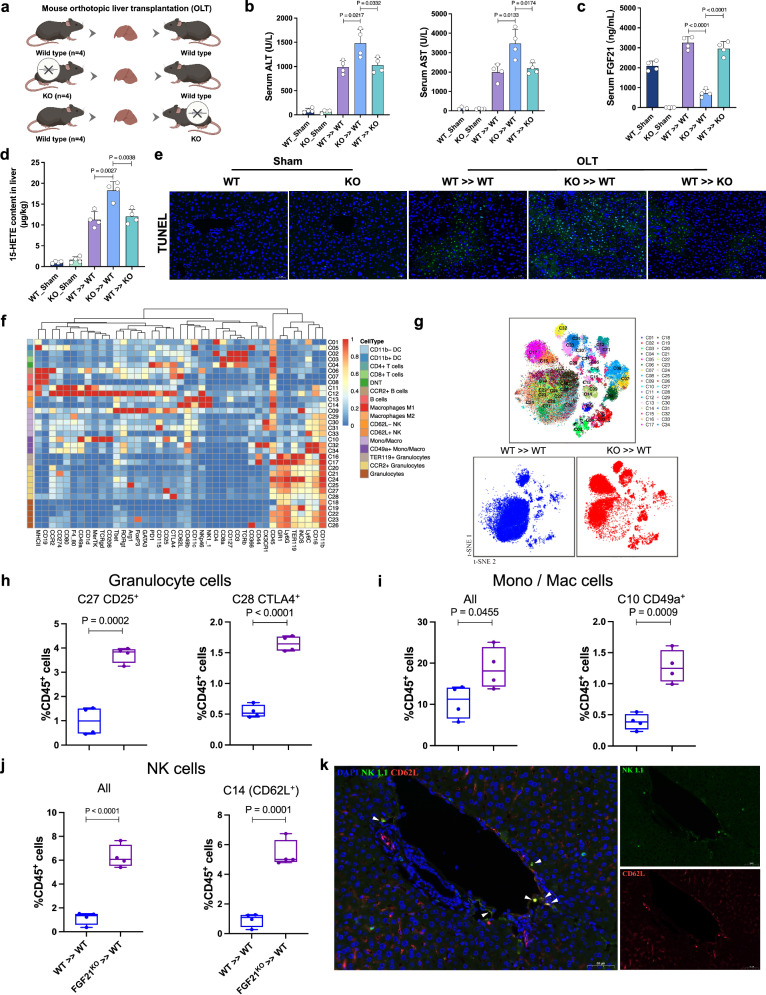
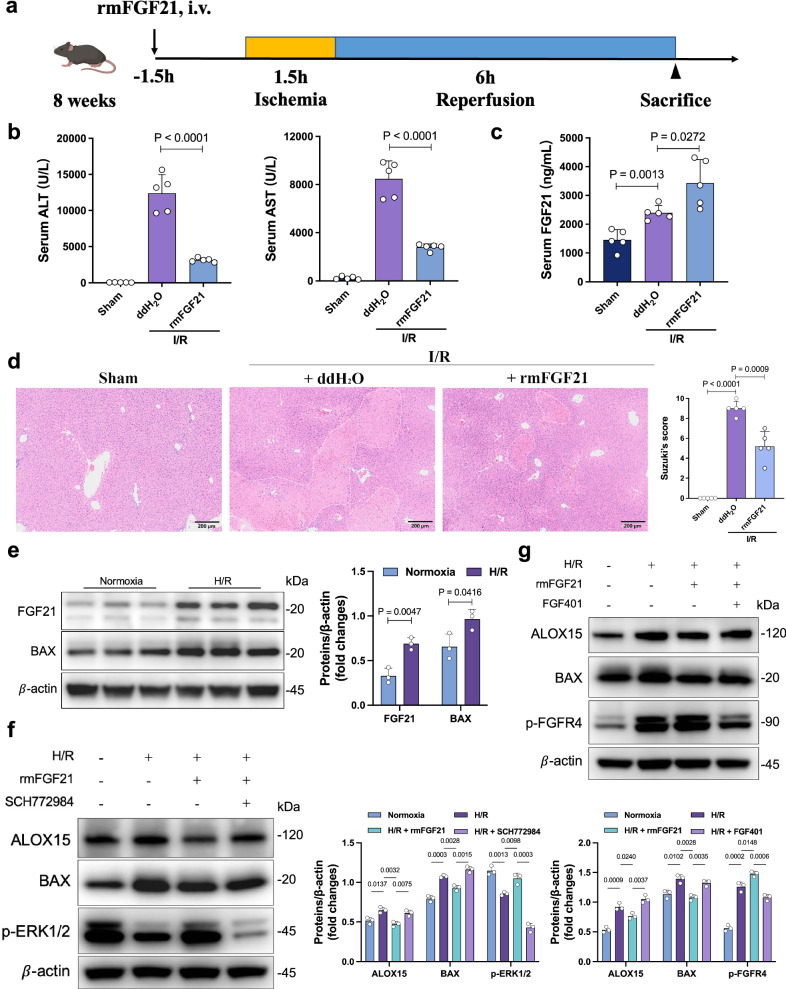
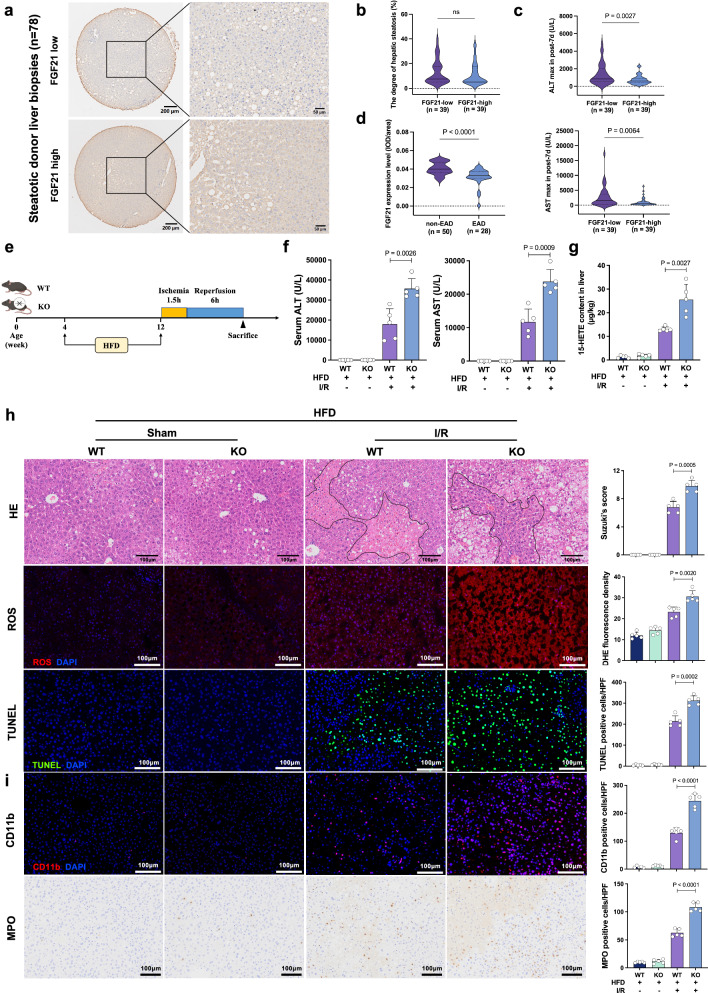
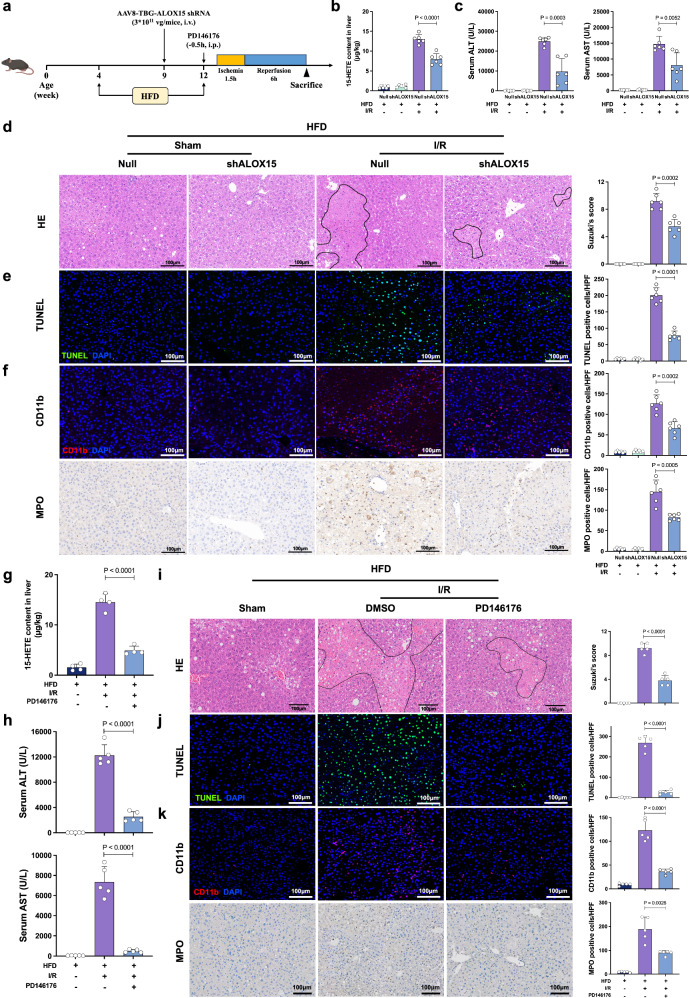
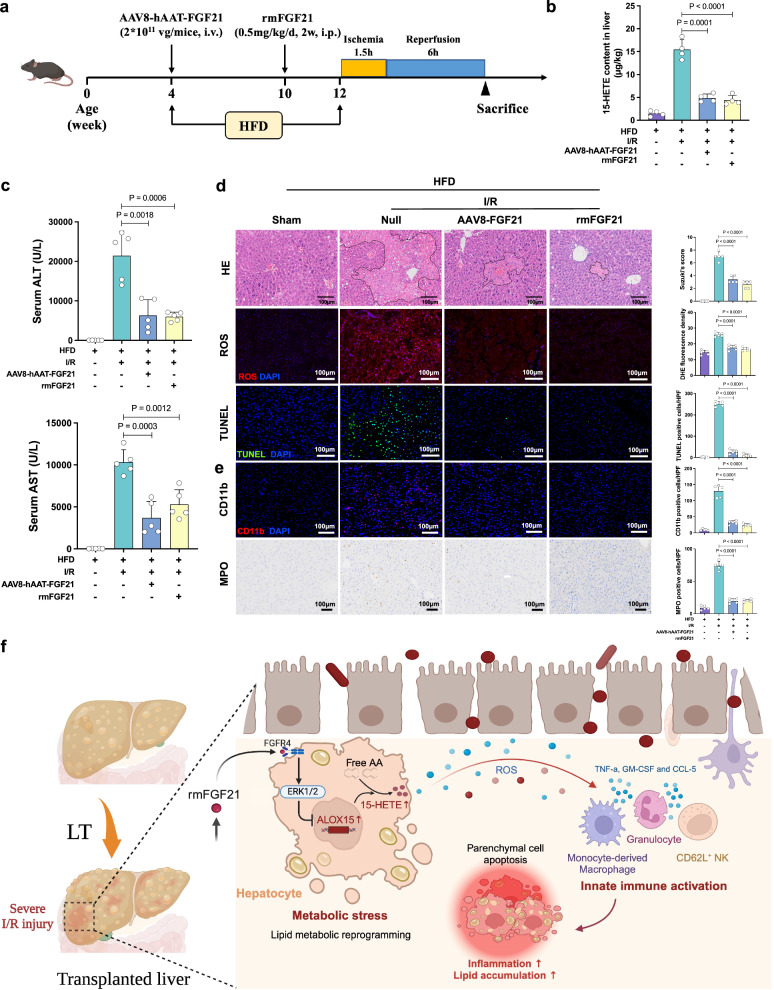
Fibroblast growth factor 21 (FGF21) is essential for modulating hepatic homeostasis, but the impact of FGF21 on liver graft injury remains uncertain. Here, we show that high FGF21 levels in liver graft and serum are associated with improved graft function and survival in liver transplantation (LT) recipients. FGF21 deficiency aggravates early graft injury and activates arachidonic acid metabolism and regional inflammation in male mouse models of hepatic ischemia/reperfusion (I/R) injury and orthotopic LT. Mechanistically, FGF21 deficiency results in abnormal activation of the arachidonate 15-lipoxygenase (ALOX15)/15-hydroxy eicosatetraenoic acid (15-HETE) pathway, which triggers a cascade of innate immunity-dominated pro-inflammatory responses in grafts. Notably, the modulating role of FGF21/ALOX15/15-HETE pathway is more significant in steatotic livers. In contrast, pharmacological administration of recombinant FGF21 effectively protects against hepatic I/R injury. Overall, our study reveals the regulatory mechanism of FGF21 and offers insights into its potential clinical application in early liver graft injury after LT.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Agopian, V. et al. Multicenter validation of the liver graft assessment following transplantation (L-GrAFT) score for assessment of early allograft dysfunction. J. Hepatol.10.1016/j.jhep.2020.09.015 (2020). - PubMed
-
- Hirao, H., Nakamura, K. & Kupiec-Weglinski, J. W. Liver ischaemia-reperfusion injury: a new understanding of the role of innate immunity. Nat. Rev. Gastroenterol. Hepatol.10.1038/s41575-021-00549-8 (2021). - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- figshare/10.6084/m9.figshare.26403022.v1
LinkOut - more resources
Full Text Sources
Medical
