

Acute kidney injury developed in the intensive care unit: a population-based prospective cohort study in the Brazilian Amazon
- PMID: 39362971
- PMCID: PMC11452208
- DOI: 10.1038/s41598-024-74177-y
Acute kidney injury developed in the intensive care unit: a population-based prospective cohort study in the Brazilian Amazon
Abstract
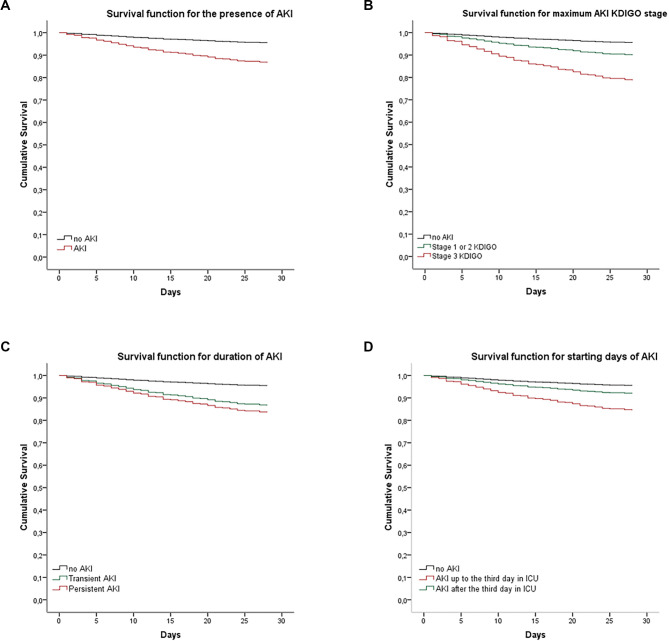
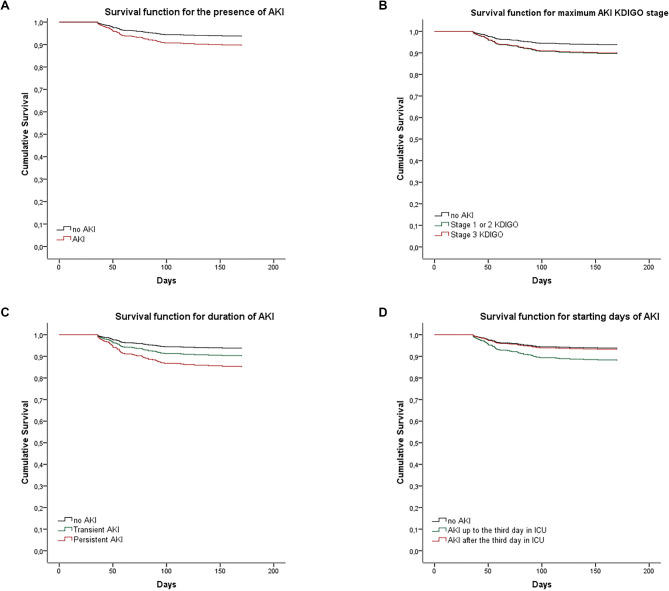
The Brazilian Amazon is a vast area with limited health care resources. To assess the epidemiology of critically ill acute kidney injury (AKI) patients in this area, a prospective cohort study of 1029 adult patients of the three intensive care units (ICUs) of Rio Branco city, the capital of Acre state, were evaluated from February 2014 to February 2016. The incidence of AKI was 53.3%. Risk factors for AKI included higher age, nonsurgical patients, admission to the ICU from the ward, higher Acute Physiology and Chronic Health Evaluation (APACHE) II scores at ICU admission, and positive fluid balance > 1500 ml/24 hours in the days before AKI development in the ICU, with aOR of 1.3 (95% CI 1.03-1.23), 1.47 (95% CI 1.07-2.03), 1.96 (95% CI 1.40-2.74), 1.05 (95% CI 1.03-1.08) for each unit increase, and 1.62 (95% CI 1.16-2.26), respectively. AKI was associated with higher ICU mortality (aOR 2.03, 95% CI 1.29-3.18). AKI mortality was independently associated with higher age, nonsurgical patients, sepsis at ICU admission, presence of shock or use of vasoactive drugs, mechanical ventilation and mean positive fluid balance in the ICU > 1500 ml/24 hours, both during ICU follow-up, with aOR 1.27 (95% CI 1.14-1.43) for each 10-year increase, 1.64 (95% CI 1.07-2.52), 2.35 (95% CI 1.14-4.83), 1.88 (95% CI 1.03-3.44), 6.73 (95% CI 4.08-11.09), 2.31 (95% CI 1.52-3.53), respectively. Adjusted hazard ratios for AKI mortality 30 and 31-180 days after ICU discharge were 3.13 (95% CI 1.84-5.31) and 1.69 (95% CI 0.99-2.90), respectively. AKI incidence was strikingly high among critically ill patients in the Brazilian Amazon. The AKI etiology, risk factors and outcomes were similar to those described in high-income countries, but mortality rates were higher.
Keywords: Acute kidney injury; Amazon; Critically ill patients; Disadvantaged populations; Epidemiology; Low-income and middle-income countries.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Risk factors and outcome of acute kidney injury in critically ill patients with SARS-CoV-2 pneumonia: a multicenter study.Med Intensiva (Engl Ed). 2025 Jan;49(1):15-24. doi: 10.1016/j.medine.2024.06.022. Epub 2024 Jul 12. Med Intensiva (Engl Ed). 2025. PMID: 39003118
-
Clinical characteristics and outcome of critically ill COVID-19 patients with acute kidney injury: a single centre cohort study.BMC Nephrol. 2021 Mar 15;22(1):92. doi: 10.1186/s12882-021-02296-z. BMC Nephrol. 2021. PMID: 33722189 Free PMC article.
-
Acute kidney injury in an intensive care unit of a general hospital with emergency room specializing in trauma: an observational prospective study.BMC Nephrol. 2015 Mar 19;16:30. doi: 10.1186/s12882-015-0026-4. BMC Nephrol. 2015. PMID: 25885883 Free PMC article.
-
Incidence and risk factors of acute kidney injury in critically ill patients from a single centre in Brazil: a retrospective cohort analysis.Sci Rep. 2019 Dec 2;9(1):18141. doi: 10.1038/s41598-019-54674-1. Sci Rep. 2019. PMID: 31792326 Free PMC article.
-
Prevention and management of antibiotic associated acute kidney injury in critically ill patients: new insights.Curr Opin Crit Care. 2023 Dec 1;29(6):595-606. doi: 10.1097/MCC.0000000000001099. Epub 2023 Sep 26. Curr Opin Crit Care. 2023. PMID: 37861206 Review.
References
-
- Komaru, Y. et al. Inverse correlation between incidence and mortality of acute kidney injury in critically ill patients: a systematic review. Shock54 (3), 280–284 (2020). - PubMed
-
- Hoste, E. A. et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med.41 (8), 1411–1423 (2015). - PubMed
-
- Hoste, E. A. J. et al. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol.14 (10), 607–625 (2018). - PubMed
