

Leveraging programmed cell death signature to predict clinical outcome and immunotherapy benefits in postoperative bladder cancer
- PMID: 39363008
- PMCID: PMC11450150
- DOI: 10.1038/s41598-024-73571-w
Leveraging programmed cell death signature to predict clinical outcome and immunotherapy benefits in postoperative bladder cancer
Abstract
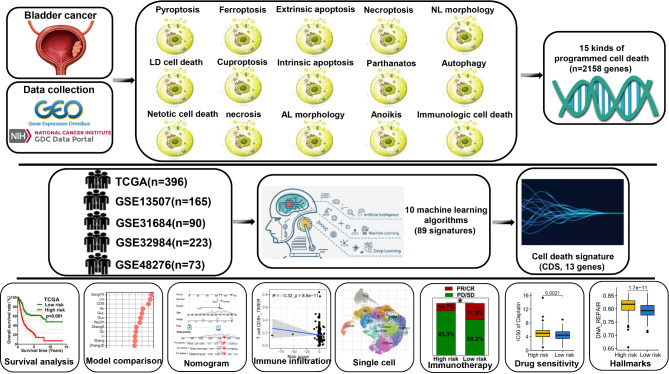
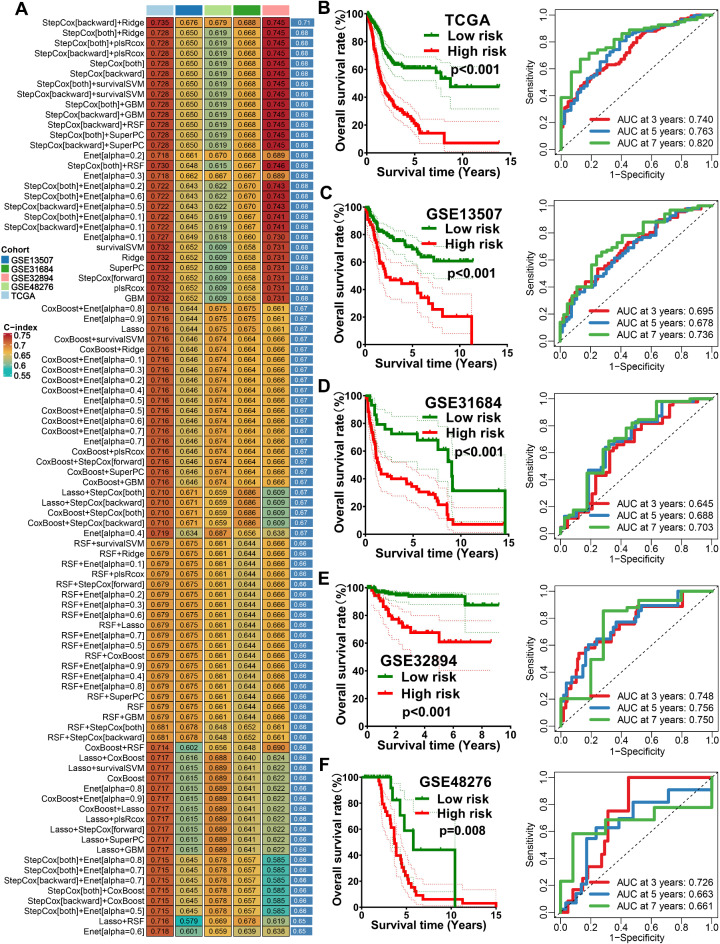
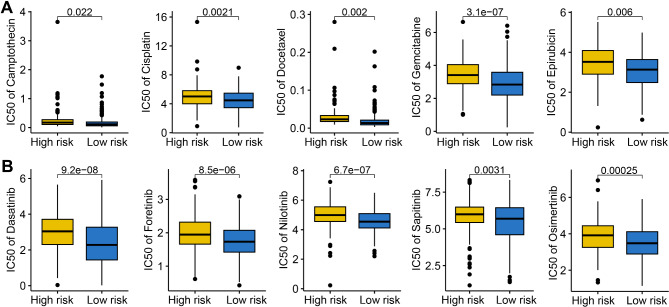
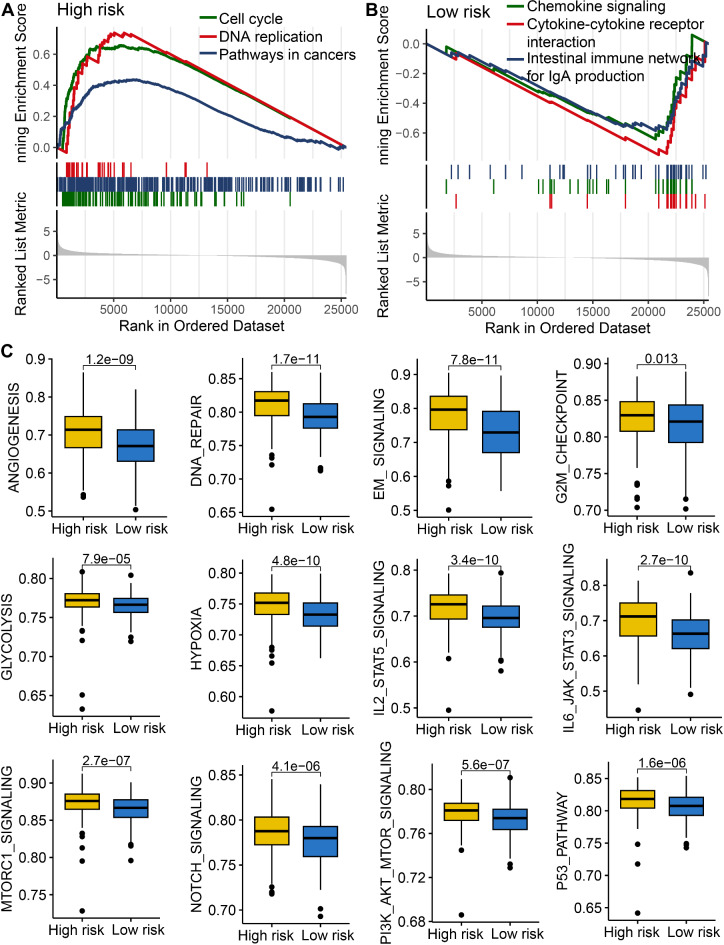
Bladder cancer is the fourth most common malignancy in men with poor prognosis. Programmed cell death (PCD) exerts crucial functions in many biological processes and immunotherapy responses of cancers. Cell death signature (CDS) is novel gene signature comprehensively considering the characteristics of 15 patterns of programmed cell death, which could affect the prognosis and immunotherapy benefits of cancer patients. Integrative machine learning procedure including 10 algorithms was conducted to construct a prognostic CDS using TCGA, GSE13507, GSE31684, GSE32984 and GSE48276 datasets. Immunophenoscore, intratumor heterogeneity (ITH), tumor immune dysfunction and exclusion (TIDE) score and five immunotherapy cohorts were used to evaluate the predictive value of CDS in immunotherapy response. The prognostic CDS constructed by StepCox[backward] + Ridge algorithms was regarded as the optimal prognostic model. The CDS had a stable and powerful performance in predicting overall survival of bladder cancer patients with the AUCs at 3-year, 5-year, and 7-year ROC of 0.740, 0.763 and 0.820 in TCGA cohort. Moreover, CDS score acted as an independent risk factor for overall survival rate of bladder cancer patients. Low CDS score had a higher abundance of immuno-activated cells, higher PD1&CTLA4 immunophenoscore, higher TMB score, lower TIDE score, lower immune escape score, lower ITH score, lower cancer-related hallmarks score in bladder cancer. The CDS score was higher in non-responders in pan-cancer patients receiving immunotherapy. Our study constructed a novel prognostic CDS, which could serve as an indicator for predicting the prognosis in postoperative bladder cancer cases and immunotherapy benefits in pan-cancer. Low CDS score indicated a better prognosis and immunotherapy benefits.
Keywords: Bladder cancer; Immunotherapy; Machine learning; Prognostic signature; Programmed cell death.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Machine learning developed an intratumor heterogeneity signature for predicting clinical outcome and immunotherapy benefit in bladder cancer.Transl Androl Urol. 2024 Jul 31;13(7):1104-1117. doi: 10.21037/tau-24-5. Epub 2024 Jul 11. Transl Androl Urol. 2024. PMID: 39100839 Free PMC article.
-
Machine learning developed immune-related exosome signature for prognosis and immunotherapy benefit in bladder cancer.Discov Oncol. 2025 Apr 18;16(1):557. doi: 10.1007/s12672-025-02354-0. Discov Oncol. 2025. PMID: 40249571 Free PMC article.
-
Machine Learning Developed a Programmed Cell Death Signature for Predicting Prognosis, Ecosystem, and Drug Sensitivity in Ovarian Cancer.Anal Cell Pathol (Amst). 2023 Oct 11;2023:7365503. doi: 10.1155/2023/7365503. eCollection 2023. Anal Cell Pathol (Amst). 2023. PMID: 37868825 Free PMC article.
-
Machine learning developed a programmed cell death signature for predicting prognosis and immunotherapy benefits in lung adenocarcinoma.Transl Oncol. 2023 Dec;38:101784. doi: 10.1016/j.tranon.2023.101784. Epub 2023 Sep 16. Transl Oncol. 2023. PMID: 37722290 Free PMC article.
-
Bladder cancer immune-related markers: diagnosis, surveillance, and prognosis.Front Immunol. 2024 Nov 4;15:1481296. doi: 10.3389/fimmu.2024.1481296. eCollection 2024. Front Immunol. 2024. PMID: 39559360 Free PMC article. Review.
Cited by
-
A comprehensive investigation of associations between cell death pathways and molecular and clinical features in pan-cancer.Clin Transl Oncol. 2025 Jun;27(6):2731-2749. doi: 10.1007/s12094-024-03769-x. Epub 2024 Nov 2. Clin Transl Oncol. 2025. PMID: 39487950
-
Machine learning-based integration develops relapse related signature for predicting prognosis and indicating immune microenvironment infiltration in breast cancer.Sci Rep. 2025 Jun 5;15(1):19773. doi: 10.1038/s41598-025-03423-8. Sci Rep. 2025. PMID: 40473720 Free PMC article.
References
-
- Lenis, A. T., Lec, P. M., Chamie, K. & Mshs, M. D. Bladder Cancer: Rev. Jama 324, 1980–1991, doi:10.1001/jama.2020.17598 (2020). - PubMed
-
- Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. Cancer J. Clin. 71, 209–249. 10.3322/caac.21660 (2021). - PubMed
-
- Lobo, N. et al. Epidemiology, screening, and Prevention of bladder Cancer. Eur. Urol. Oncol. 5, 628–639. 10.1016/j.euo.2022.10.003 (2022). - PubMed
-
- Li, Z. et al. Oncogene Mir-187-5p is associated with cellular proliferation, migration, invasion, apoptosis and an increased risk of recurrence in bladder cancer. Biomed. Pharmacotherapy = Biomedecine Pharmacotherapie. 105, 461–469. 10.1016/j.biopha.2018.05.122 (2018). - PubMed
-
- Compérat, E. et al. Current best practice for bladder cancer: a narrative review of diagnostics and treatments. Lancet (London England). 400, 1712–1721. 10.1016/s0140-6736(22)01188-6 (2022). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
