

Placental extracellular vesicles promote cardiomyocyte maturation and fetal heart development
- PMID: 39363116
- PMCID: PMC11450004
- DOI: 10.1038/s42003-024-06938-4
Placental extracellular vesicles promote cardiomyocyte maturation and fetal heart development
Abstract
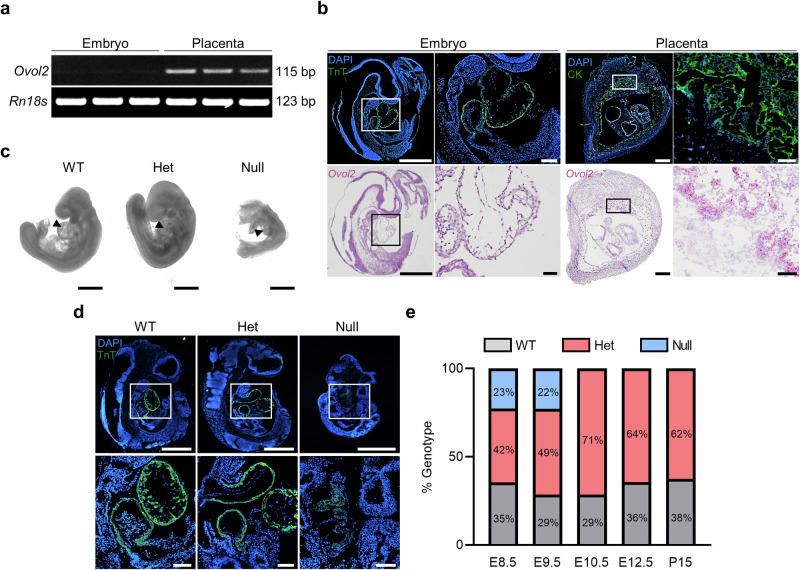
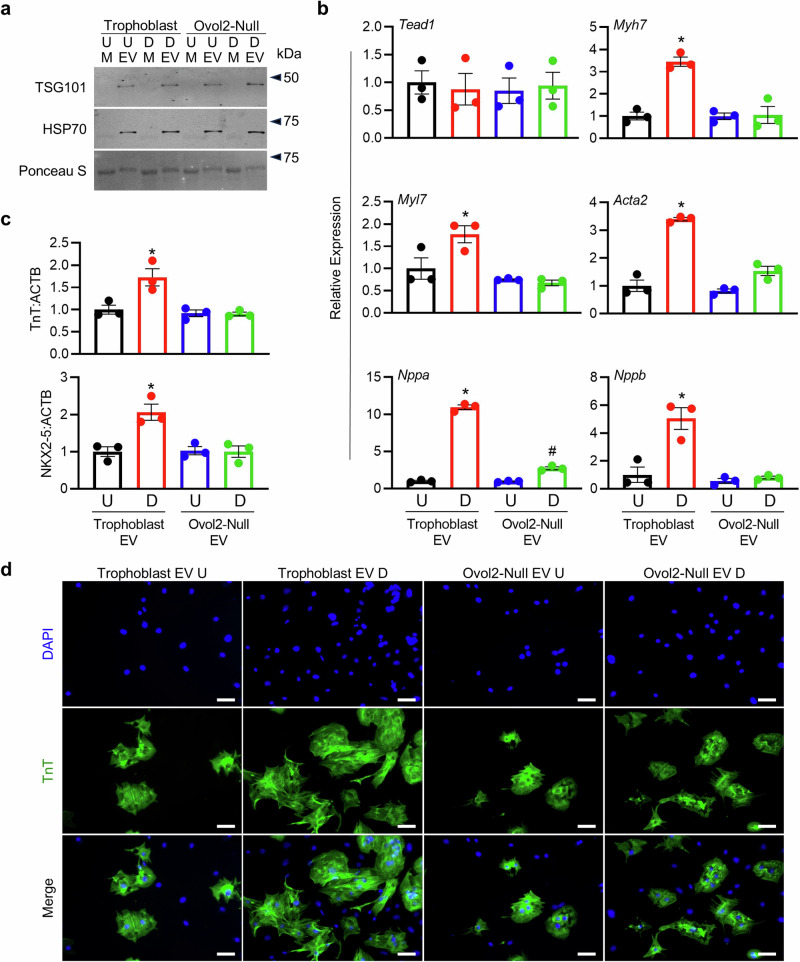
Congenital heart defects are leading causes of neonatal mortality and are often associated with placental abnormalities, but mechanisms linking placenta and heart development are poorly understood. Herein, we investigated a potential signaling network connecting the placenta and nascent heart in mice. We found that fetal hearts exposed to media conditioned by placental tissue or differentiated wild-type trophoblast stem (TS) cells, but not undifferentiated TS cells, showed increased heart rate and epicardial cell outgrowth. This effect was not observed when hearts were exposed to media from TS cells lacking OVO-Like 2, a transcription factor required for trophoblast differentiation and placental development. Trophoblasts released abundant extracellular vesicles into media, and these vesicles were sufficient to mediate cardio-promoting effects. Our findings provide a potential mechanism whereby the placenta communicates with the fetal heart to promote cardiac morphogenesis, and offers insight into the link between poor placentation and a higher incidence of heart defects.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Seo, D. M. et al. The outcome of open heart surgery for congenital heart disease in infants with low body weight less than 2500 g. Pediatr. Cardiol.32, 578–584 (2011). - PubMed
-
- Suluba, E., Shuwei, L., Xia, Q. & Mwanga, A. Congenital heart diseases: genetics, non-inherited risk factors, and signaling pathways. Egypt. J. Med. Hum. Genet. 2020 21121, 1–12 (2020).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
