

Clinical, developmental and serotonemia phenotyping of a sample of 70 Italian patients with Phelan-McDermid Syndrome
- PMID: 39363263
- PMCID: PMC11451156
- DOI: 10.1186/s11689-024-09572-7
Clinical, developmental and serotonemia phenotyping of a sample of 70 Italian patients with Phelan-McDermid Syndrome
Abstract
Background: Phelan-McDermid syndrome (PMS) is caused by monoallelic loss or inactivation at the SHANK3 gene, located in human chr 22q13.33, and is often associated with Autism Spectrum Disorder (ASD).
Objectives: To assess the clinical and developmental phenotype in a novel sample of PMS patients, including for the first time auxometric trajectories and serotonin blood levels.
Methods: 70 Italian PMS patients were clinically characterized by parental report, direct medical observation, and a thorough medical and psychodiagnostic protocol. Serotonin levels were measured in platelet-rich plasma by HPLC.
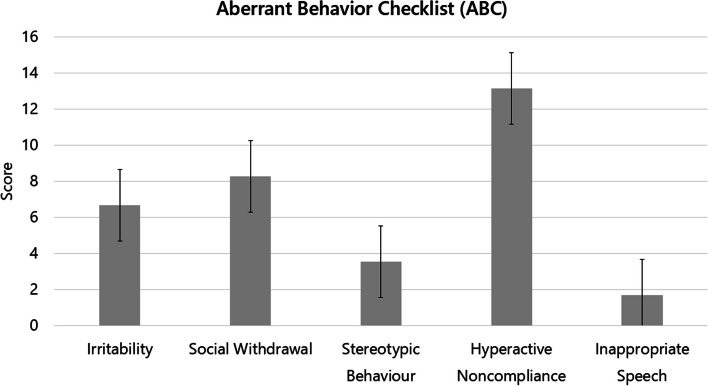
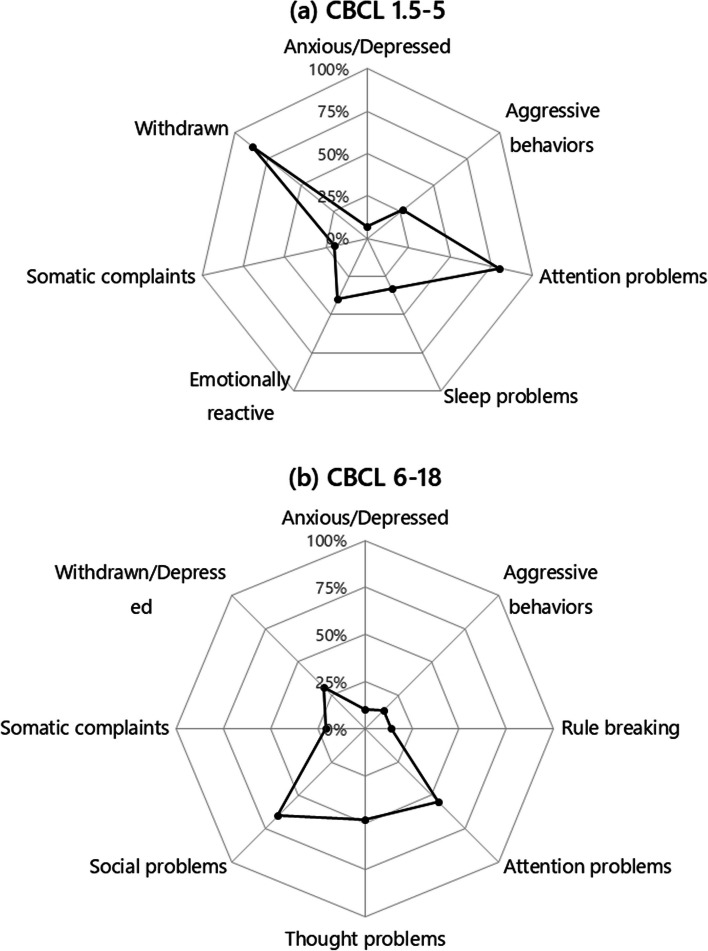
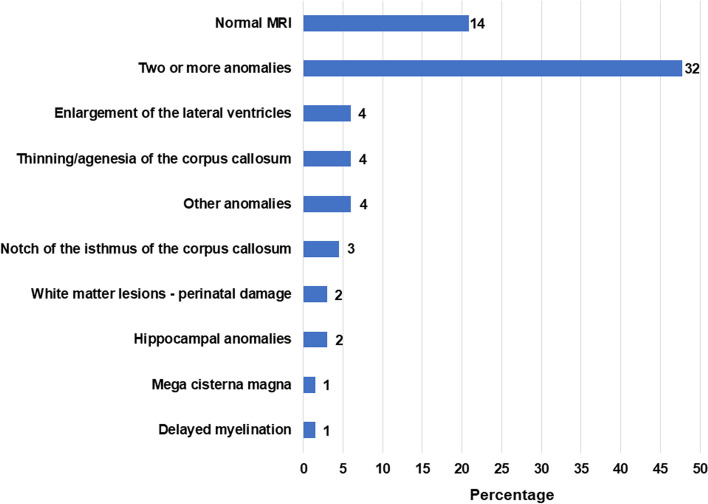
Results: Our sample includes 59 (84.3%) cases with chr. 22q13 terminal deletion, 5 (7.1%) disruptive SHANK3 mutations, and 6 (8.6%) ring chromosome 22. Intellectual disability was present in 69 (98.6%) cases, motor coordination disorder in 65 (92.9%), ASD in 20 (28.6%), and lifetime bipolar disorder in 12 (17.1%). Prenatal and postnatal complications were frequent (22.9%-48.6%). Expressive and receptive language were absent in 49 (70.0%) and 19 (27.1%) cases, respectively. Decreased pain sensitivity was reported in 56 (80.0%), hyperactivity in 49 (80.3%), abnormal sleep in 45 (64.3%), congenital dysmorphisms in 35 (58.3%), chronic stool abnormalities and especially constipation in 29 (41.4%). Parents reported noticing behavioral abnormalities during early childhood immediately after an infective episode in 34 (48.6%) patients. Brain MRI anomalies were observed in 53 (79.1%), EEG abnormalities in 16 (23.5%), kidney and upper urinary tract malformations in 18 (28.1%). Two novel phenotypes emerged: (a) a subgroup of 12/44 (27.3%) PMS patients displays smaller head size at enrollment (mean age 11.8 yrs) compared to their first year of neonatal life, documenting a deceleration of head growth (p < 0.001); (b) serotonin blood levels are significantly lower in 21 PMS patients compared to their 21 unaffected siblings (P < 0.05), and to 432 idiopathic ASD cases (p < 0.001).
Conclusions: We replicate and extend the description of many phenotypic characteristics present in PMS, and report two novel features: (1) growth trajectories are variable and head growth appears to slow down during childhood in some PMS patients; (2) serotonin blood levels are decreased in PMS, and not increased as frequently occurs in ASD. Further investigations of these novel features are under way.
Keywords: SHANK3; 22q13 deletion syndrome; Autism spectrum disorder; Hyperserotonemia; Intellectual disability; Macrocephaly; Neuroinflammation; Phelan-McDermid syndrome; Phenotype; Serotonin.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests
Figures


References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
