

Deciphering resistance mechanisms in cancer: final report of MATCH-R study with a focus on molecular drivers and PDX development
- PMID: 39363320
- PMCID: PMC11451117
- DOI: 10.1186/s12943-024-02134-4
Deciphering resistance mechanisms in cancer: final report of MATCH-R study with a focus on molecular drivers and PDX development
Abstract
Background: Understanding the resistance mechanisms of tumor is crucial for advancing cancer therapies. The prospective MATCH-R trial (NCT02517892), led by Gustave Roussy, aimed to characterize resistance mechanisms to cancer treatments through molecular analysis of fresh tumor biopsies. This report presents the genomic data analysis of the MATCH-R study conducted from 2015 to 2022 and focuses on targeted therapies.
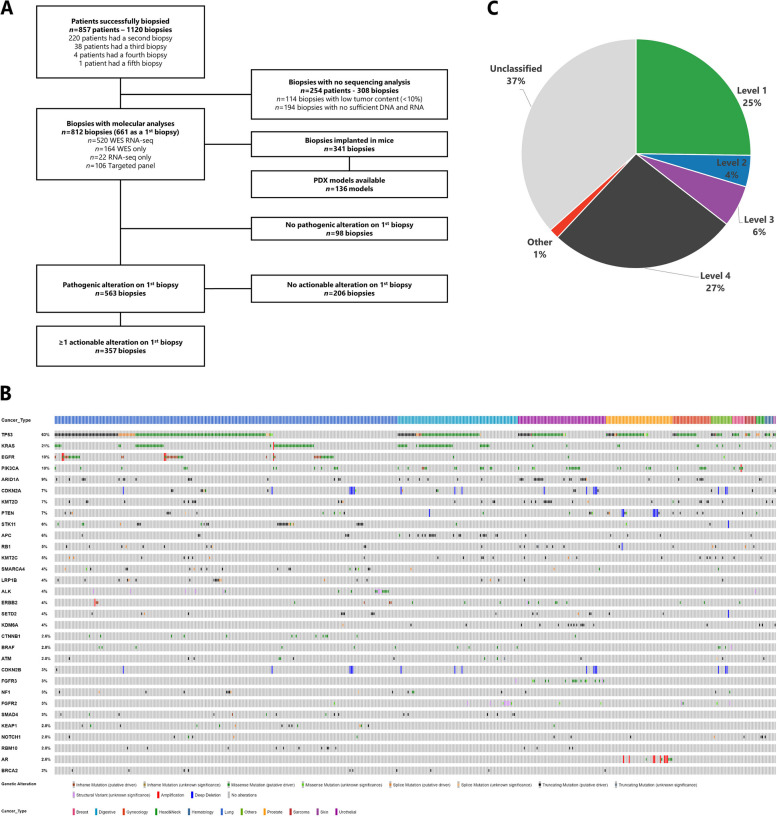
Methods: The study included resistant metastatic patients (pts) who accepted an image-guided tumor biopsy. After evaluation of tumor content (TC) in frozen tissue biopsies, targeted NGS (10 < TC < 30%) or Whole Exome Sequencing and RNA sequencing (TC > 30%) were performed before and/or after the anticancer therapy. Patient-derived xenografts (PDX) were established by implanting tumor fragments into NOD scid gamma mice and amplified up to five passages.
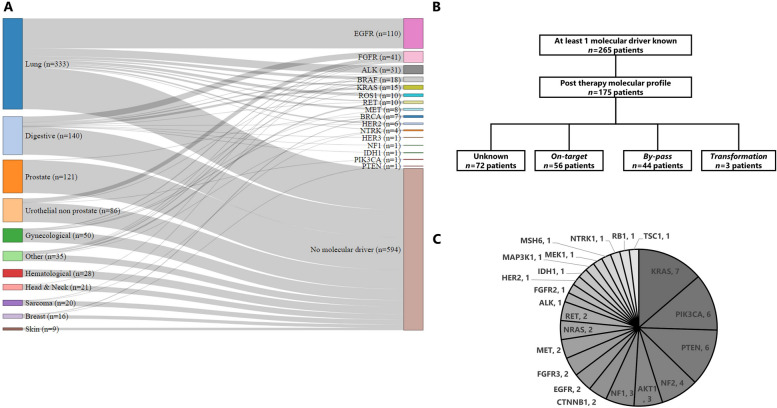
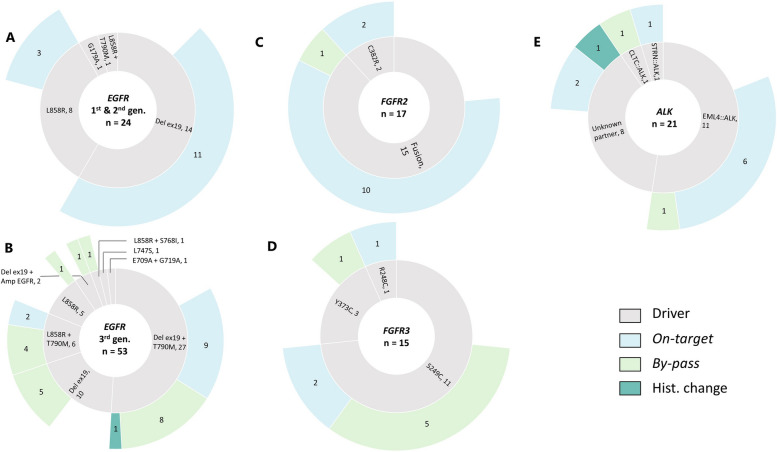
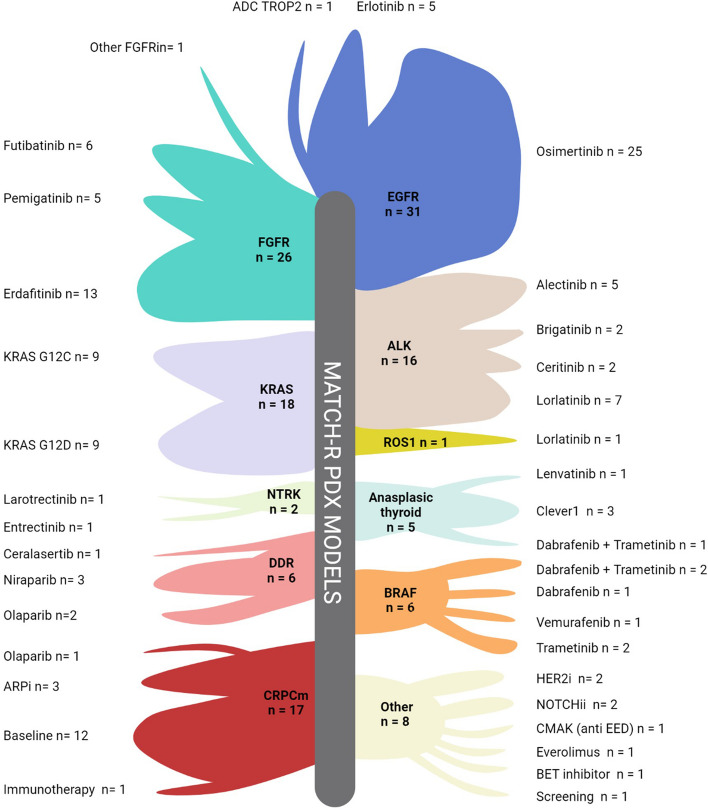
Results: A total of 1,120 biopsies were collected from 857 pts with the most frequent tumor types being lung (38.8%), digestive (16.3%) and prostate (14.1%) cancer. Molecular targetable driver were identified in 30.9% (n = 265/857) of the patients, with EGFR (41.5%), FGFR2/3 (15.5%), ALK (11.7%), BRAF (6.8%), and KRAS (5.7%) being the most common altered genes. Furthermore, 66.0% (n = 175/265) had a biopsy at progression on targeted therapy. Among resistant cases, 41.1% (n = 72/175) had no identified molecular mechanism, 32.0% (n = 56/175) showed on-target resistance, and 25.1% (n = 44/175) exhibited a by-pass resistance mechanism. Molecular profiling of the 44 patients with by-pass resistance identified 51 variants, with KRAS (13.7%), PIK3CA (11.8%), PTEN (11.8%), NF2 (7.8%), AKT1 (5.9%), and NF1 (5.9%) being the most altered genes. Treatment was tailored for 45% of the patients with a resistance mechanism identified leading to an 11 months median extension of clinical benefit. A total of 341 biopsies were implanted in mice, successfully establishing 136 PDX models achieving a 39.9% success rate. PDX models are available for EGFR (n = 31), FGFR2/3 (n = 26), KRAS (n = 18), ALK (n = 16), BRAF (n = 6) and NTRK (n = 2) driven cancers. These models closely recapitulate the biology of the original tumors in term of molecular alterations and pharmacological status, and served as valuable models to validate overcoming treatment strategies.
Conclusion: The MATCH-R study highlights the feasibility of on purpose image guided tumor biopsies and PDX establishment to characterize resistance mechanisms and guide personalized therapies to improve outcomes in pre-treated metastatic patients.
Keywords: Biopsy; Cancer; Metastatic; PDX; Resistance; Targeted therapy.
© 2024. The Author(s).
Conflict of interest statement
D. Vasseur: speaker for Roche and Astra Zeneca JC. Soria: Full time employee of Amgen. Share-holder of Amgen. LF: Research funding from Debiopharm, Incyte, Relay Therapeutics, Sanofi and Nuvalent. F. Facchinetti : personal fees from BeiGene outside the submitted work. Y. Loriot : personal fees, nonfinancial support, and other support from Janssen during the conduct of the study, as well as personal fees, nonfinancial support, and other support from MSD, Pfizer, Merck KGaA, Astellas, Gilead, Bristol Myers Squibb, and Roche, nonfinancial support and other support from Incyte, other support from Exelixis, and personal fees and other support from Taiho outside the submitted work. S. Michiels : personal fees from DSMB or scientific committee study membership for Kedrion, Biophytis, Servier, IQVIA, Yuhan, and Roche outside the submitted work. L. Tselikas : personal fees from Incyte during the conduct of the study, as well as personal fees from GE Healthcare, Quantum Surgical, and Boston Scientific outside the submitted work. B. Besse : other support from AbbVie, BioNTech SE, Bristol Myers Squibb, Chugai Pharmaceutical, CureVac AG, Daiichi Sankyo, F. Hoffmann-La Roche Ltd, PharmaMar, Regeneron, Sanofi-Aventis, and Turning Point Therapeutics, other support from AbbVie, Eli Lilly and Company, Ellipses Pharma Ltd, F.Hoffmann-La Roche Ltd, Genmab, Immunocore, Janssen, MSD, Ose Immunotherapeutics, Owkin, and Taiho oncology, other support from AstraZeneca, BeiGene, Genmab A/S, GlaxoSmithKline, Janssen, MSD, Ose Immunotherapeutics, PharmaMar, Roche-Genentech, Sanofi, and Takeda, and other support from AbbVie, AstraZeneca, Chugai Pharmaceutical, Daichii Sankyo, Hedera Dx, Janssen, MSD, Roche, Sanofi-Aventis, and Springer Healthcare Ltd during the conduct of the study. F. André : grants from AstraZeneca, Guardant Health, Novartis, Owkin, Pfizer, Eli Lilly and Company, Roche, and Daiichi Sankyo, other support from Boston Pharmaceutics, Gilead, and Servier, and grants and other support from N-Power medicine outside the submitted work. A. Hollebecque : personal fees and nonfinancial support from Amgen, personal fees from Basilea, Bristol Myers and Squibb, Servier, Relay Therapeutics, Taiho, MSD, Seagen, grants and personal fees from Incyte, and nonfinancial support from Pierre Fabre outside the submitted work, as well as reports being a PI of the TransThera (Tinengotinib) phase III trial. A. Gazzah: travel accommodations, congress registration expenses from Boehringer Ingelheim, Novartis, Pfizer, and Roche. Consultant/Expert role for Novartis. Principal/sub-Investigator of Clinical Trials for Aduro Biotech, Agios Pharmaceuticals, Amgen, Argen-X Bvba, Arno Therapeutics, Astex Pharmaceuticals, Astra Zeneca, Aveo, Bayer Healthcare Ag, Bbb Technologies Bv, Beigene, Bioalliance Pharma, Biontech Ag, Blueprint Medicines, Boehringer Ingelheim, Bristol Myers Squibb, Ca, Celgene Corporation, Chugai Pharmaceutical Co., Clovis Oncology, Daiichi Sankyo, Debiopharm S.A., Eisai, Exelixis, Forma, Gamamabs, Genentech, Inc., Gilead Sciences, Inc., GlaxoSmithKline, Glenmark Pharmaceuticals, H3 Biomedicine, Inc., Hoffmann La Roche Ag, Incyte Corporation, Innate Pharma, Iris Servier, Janssen, Kura Oncology, Kyowa Kirin Pharm, Lilly, Loxo Oncology, Lytix Biopharma As, Medimmune, Menarini Ricerche, Merck Sharp & Dohme Chibret, Merrimack Pharmaceuticals, Merus, Millennium Pharmaceuticals, Nanobiotix, Nektar Therapeutics, Novartis Pharma, Octimet Oncology Nv, Oncoethix, Oncomed, Oncopeptides, Onyx Therapeutics, Orion Pharma, Oryzon Genomics, Pfizer, Pharma Mar, Pierre Fabre, Rigontec Gmbh, Roche, Sanofi Aventis, Sierra Oncology, Taiho Pharma, Tesaro, Inc., Tioma Therapeutics, Inc., Xencor. Research Grants from AstraZeneca, BMS, Boehringer Ingelheim, Janssen Cilag, Merck, Novartis, Pfizer, Roche, Sanofi. Non-financial support (drug supplied) from AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Johnson & Johnson, Lilly, Medimmune, Merck, NH TherAGuiX, Pfizer, Roche. D. Planchard: Consulting, advisory role or lectures: AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Merck, MedImmune, Novartis, Pfizer, prIME Oncology, Peer CME, Roche. Honoraria: AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Celgene, Eli Lilly, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, Roche. Clinical trials research as principal or co-investigator (Institutional financial interests): AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Pfizer, Roche, Medimmune, Sanofi Aventis, Taiho Pharma, Novocure, and Daiichi Sanky. Travel, Accommodations, Expenses: AstraZeneca, Roche, Novartis, prIME Oncology, Pfizer. M. Aldea: Expenses from Sandoz. No disclosures were reported by the other authors.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
