

Review article: Scoping review of interventions that reduce mechanical restraint in the emergency department
- PMID: 39363492
- PMCID: PMC11744410
- DOI: 10.1111/1742-6723.14498
Review article: Scoping review of interventions that reduce mechanical restraint in the emergency department
Abstract
Objective: Mechanical restraints are known to be associated with many undesirable outcomes in clinical settings. Our objective was to examine the current literature to explore possible interventions that would reduce the use of mechanical restraints in the ED.
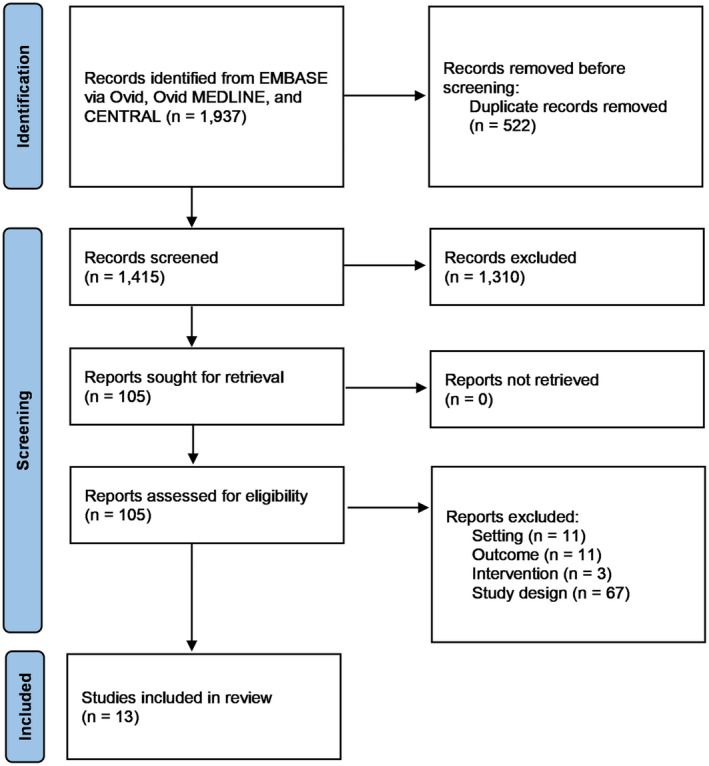
Methods: In this scoping review, we searched online databases Embase, MEDLINE and Cochrane CENTRAL for any studies published between the databases from 1 January 2007 to 19 September 2023. Studies were included if interventions were hospital- or staff-focused and reported measured outcomes before and after the introduction of the intervention. Risk of bias was assessed using the JBI Critical Appraisal Checklist for Cohort Studies.
Results: The search strategy yielded 1937 studies across the three databases, of which 13 studies were extracted and included in the review. Interventions were categorised into four groups: provision of staff training, addition of a de-escalation team, creation of a dedicated unit and introduction of an agitation scale only. Most of the studies saw reduction in restraint rates or time in restraints. Only the two studies that used an agitation scale as a stand-alone intervention saw no significant reduction. Only one study had low risk of bias, whereas the remainder had high risk.
Conclusions: Evidence supports further exploration of interventions that include: designing an agitation guideline; training staff in assessment, attitudinal and de-escalation skills; addition of a crisis team; and environmental changes in the form of adding a dedicated clinical space. Although these strategies may reduce mechanical restraint in the ED setting, further high-quality studies are needed before definitive conclusions may be drawn.
© 2024 The Author(s). Emergency Medicine Australasia published by John Wiley & Sons Australia, Ltd on behalf of Australasian College for Emergency Medicine.
Conflict of interest statement
None declared.
References
-
- Bak J, Brandt‐Christensen M, Sestoft DM, Zoffmann V. Mechanical restraint – which interventions prevent episodes of mechanical restraint? – a systematic review. Perspect. Psychiatr. Care 2012; 48: 83–94. - PubMed
-
- Mohr WK, Petti TA, Mohr BD. Adverse effects associated with physical restraint. Can. J. Psychiatry 2003; 48: 330–337. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
