

The glucocorticoid dose-mortality nexus in pneumonia patients: unveiling the threshold effect
- PMID: 39364057
- PMCID: PMC11447404
- DOI: 10.3389/fphar.2024.1445979
The glucocorticoid dose-mortality nexus in pneumonia patients: unveiling the threshold effect
Abstract
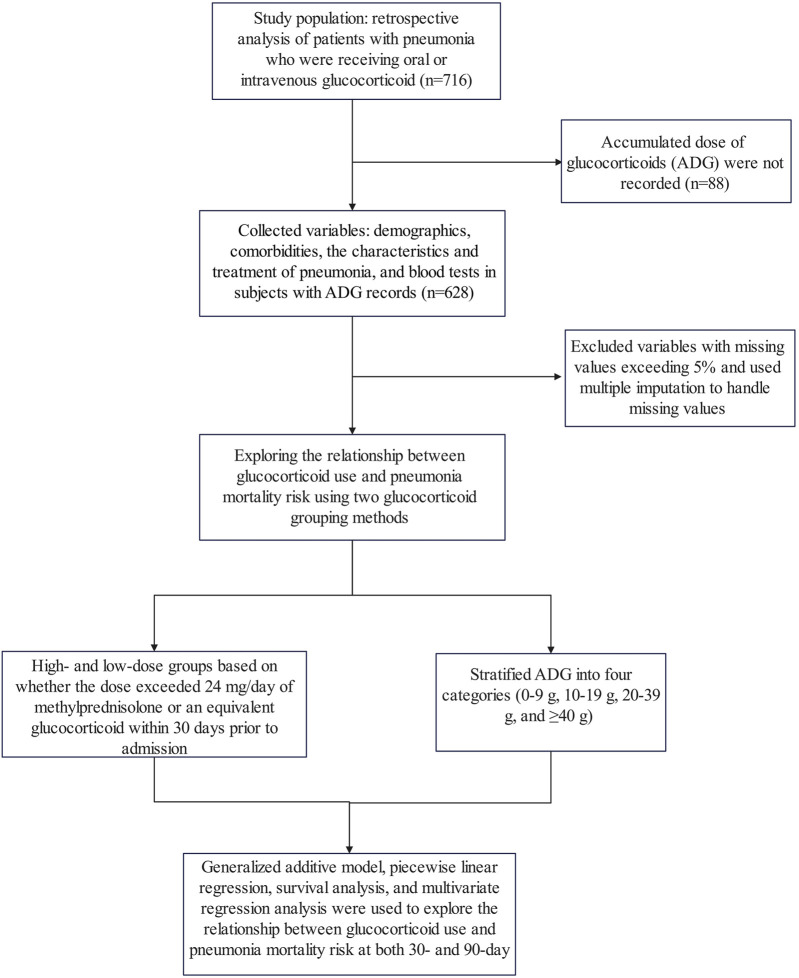
Background: The impact of glucocorticoid use on mortality risk in pneumonia patients remains unclear. This study aimed to investigate the relationship between the accumulated dose of glucocorticoids (ADG) and secondary pneumonia mortality risk among patients receiving oral or intravenous glucocorticoids.
Methods: Data from the DRYAD database were analyzed, covering pneumonia patients from six academic hospitals over a 5-year period who had been administered oral or intravenous glucocorticoids. Piecewise linear regression and multivariate regression analysis were utilized to assess the association between ADG and mortality risk in pneumonia patients, while adjusting for potential confounders.
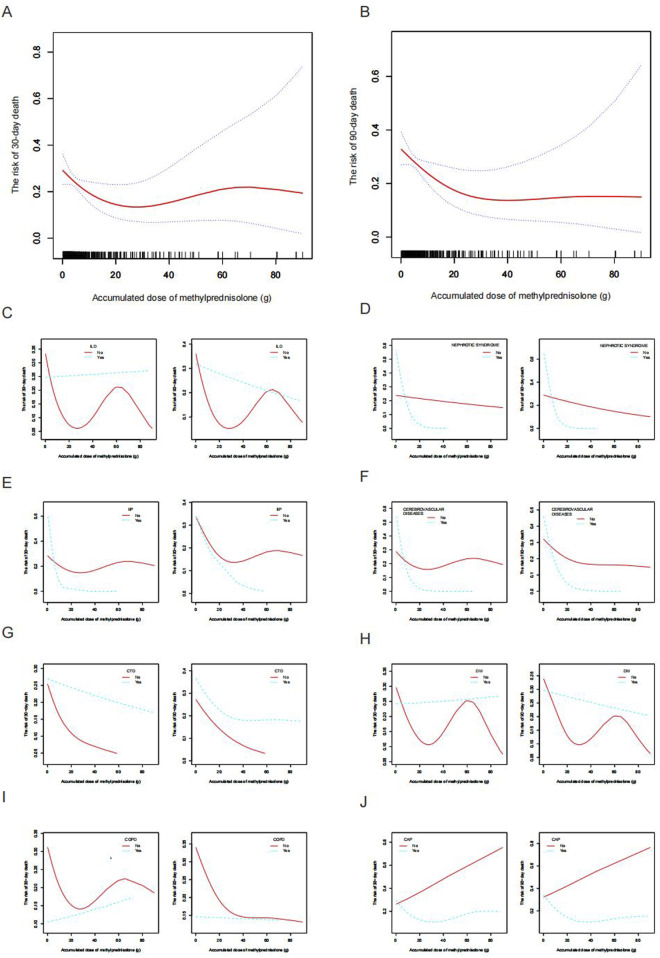
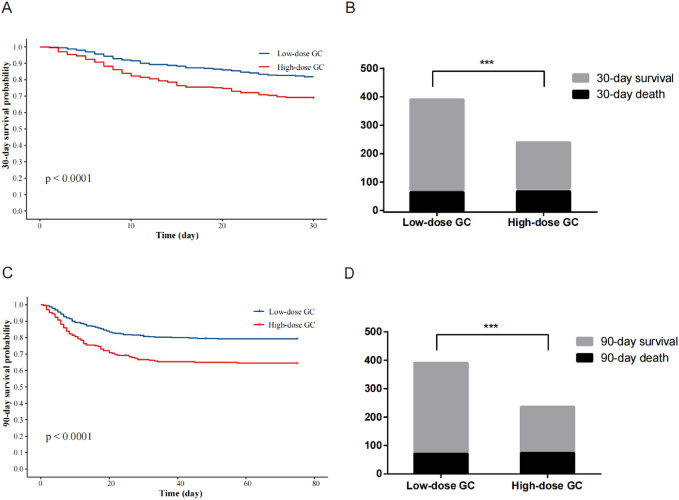
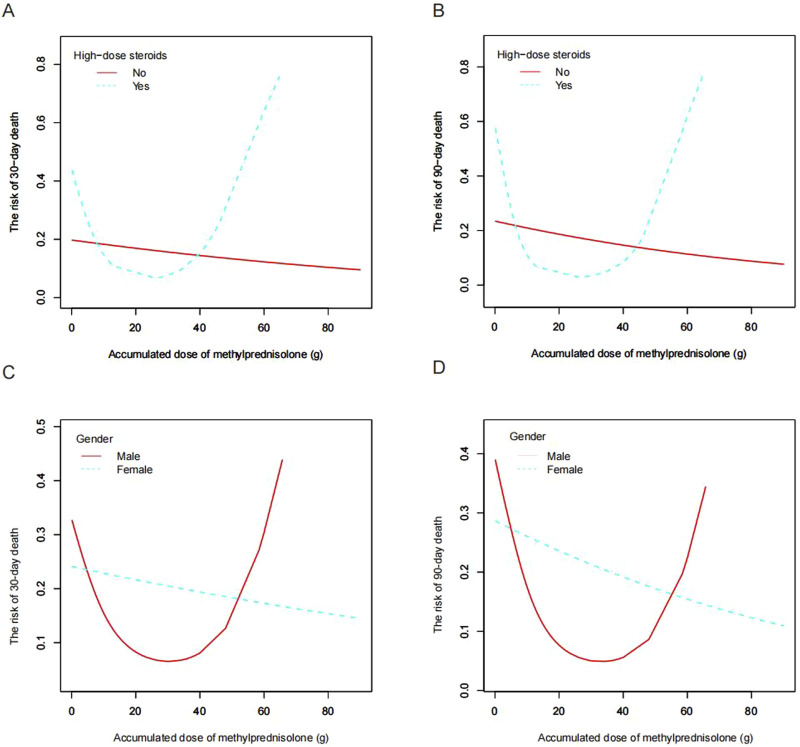
Results: Among the 628 pneumonia patients included, the 30-day mortality rate was 23.1% and the 90-day mortality rate was 26.4%. In the high-dose glucocorticoid group (≥24 mg/day of methylprednisolone or an equivalent glucocorticoid within 30 days before admission), the 30-day and 90-day mortality rates were 31.2% and 35.9%, respectively. Piecewise linear regression analysis demonstrated a non-linear relationship between ADG and mortality risk in pneumonia patients. Multivariate regression analysis revealed a significantly lower mortality risk in patients receiving an ADG of 20-39 g methylprednisolone compared to those receiving lower (<20 g) or higher doses (≥40 g), after adjusting for potential confounding factors. Additionally, in the high-dose glucocorticoid group, surpassing the inflection point of 20 g of methylprednisolone raised the 30-day and 90-day mortality risks (adjusted odds ratio, 95% confidence interval: 1.16, 1.03-1.30 and 1.23, 1.07-1.42, respectively). Notably, this threshold effect was observed exclusively in male patients.
Conclusion: This study provides evidence supporting a potential threshold effect between ADG and mortality risk in oral or intravenous glucocorticoid users with secondary pneumonia. Specifically, male patients receiving high-dose glucocorticoids should undergo close monitoring when the ADG of methylprednisolone exceeds 20 g, as it may be associated with an elevated risk of mortality.
Keywords: gender; glucocorticoids; mortality; pneumonia; threshold effect.
Copyright © 2024 Wang and Ye.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Annane D., Pastores S. M., Rochwerg B., Arlt W., Balk R. A., Beishuizen A., et al. (2017). Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive Care Med. 43 (12), 1751–1763. 10.1007/s00134-017-4919-5 - DOI - PubMed
-
- Buttgereit F., da Silva J. A., Boers M., Burmester G. R., Cutolo M., Jacobs J., et al. (2002). Standardised nomenclature for glucocorticoid dosages and glucocorticoid treatment regimens: current questions and tentative answers in rheumatology. Ann. Rheum. Dis. 61 (8), 718–722. 10.1136/ard.61.8.718 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources