

Immunoglobulin G4 in primary Sjögren's syndrome and IgG4-related disease - connections and dissimilarities
- PMID: 39364411
- PMCID: PMC11446744
- DOI: 10.3389/fimmu.2024.1376723
Immunoglobulin G4 in primary Sjögren's syndrome and IgG4-related disease - connections and dissimilarities
Abstract
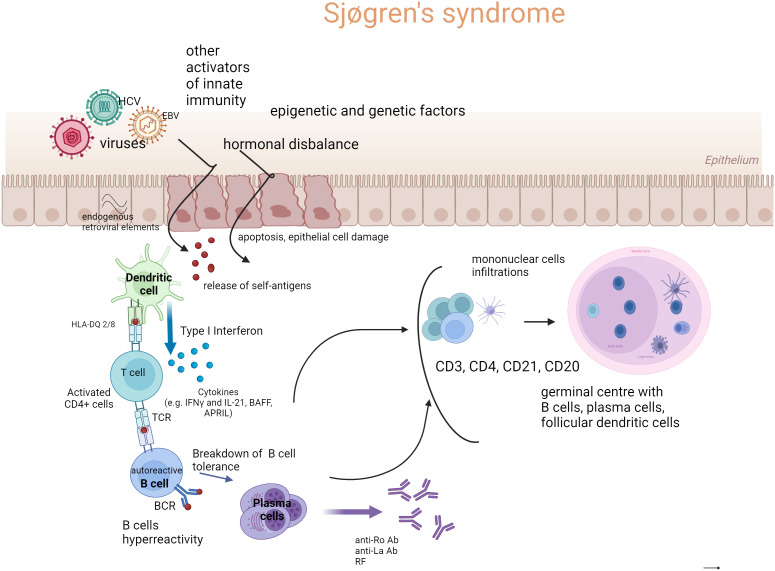
Primary Sjögren's syndrome (pSS) is an autoimmune disease, with B cell hyperactivation and autoantibody production as its immunological hallmarks. Although the distinction between immunoglobulin G4-related disease (IgG4-RD) and pSS, based on the presence or absence of certain autoantibodies, seems easy to make, possibility of elevated serum IgG4 concentration and often similar organ involvement may lead to a misdiagnosis. The increased serum concentration of IgG4 in IgG4-RD is not clearly linked to the pathogenesis of IgG-RD and it has been suggested that it may constitute just an epiphenomenon. The aim of this article is to discuss the presence of IgG4 in pSS and IgG4-RD and its potential significance for these two diseases.
Keywords: IgG4-related disease; Sjögren’s syndrome; autoimmunity; immunoglobulin G4; lymphomas.
Copyright © 2024 Maslinska and Kostyra-Grabczak.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Serum soluble interleukin-2 receptor is a useful biomarker for disease activity but not for differential diagnosis in IgG4-related disease and primary Sjögren's syndrome adults from a defined population.Clin Exp Rheumatol. 2018 May-Jun;36 Suppl 112(3):157-164. Epub 2018 Feb 15. Clin Exp Rheumatol. 2018. PMID: 29465360
-
Pathogenesis of IgG4-related disease. Comparison with Sjögren's syndrome.Mod Rheumatol. 2020 Jan;30(1):7-16. doi: 10.1080/14397595.2019.1650694. Epub 2019 Aug 19. Mod Rheumatol. 2020. PMID: 31425659 Review.
-
Serum immunoglobulin G4 in Sjögren's syndrome: a pilot study.Rheumatol Int. 2020 Apr;40(4):555-561. doi: 10.1007/s00296-020-04529-0. Epub 2020 Feb 15. Rheumatol Int. 2020. PMID: 32062697
-
Clinical Performance of Immunonephelometric Assay and Chemiluminescent Immunoassay for Detection of IgG Subclasses in Chinese.J Clin Lab Anal. 2024 Apr;38(8):e25033. doi: 10.1002/jcla.25033. Epub 2024 Apr 2. J Clin Lab Anal. 2024. PMID: 38563457 Free PMC article.
-
T helper subsets in Sjögren's syndrome and IgG4-related dacryoadenitis and sialoadenitis: a critical review.J Autoimmun. 2014 Jun;51:81-8. doi: 10.1016/j.jaut.2013.07.007. Epub 2013 Aug 3. J Autoimmun. 2014. PMID: 23920005 Review.
Cited by
-
Unraveling the complexity of IgG4-related aortitis and periarteritis: from pathogenesis to clinical practice.Front Immunol. 2025 Jul 4;16:1625456. doi: 10.3389/fimmu.2025.1625456. eCollection 2025. Front Immunol. 2025. PMID: 40688077 Free PMC article. Review.
-
IgG4-RD-Associated Mikulicz Syndrome Without Classic Systemic Involvement-A Case Report.J Clin Med. 2025 Feb 2;14(3):958. doi: 10.3390/jcm14030958. J Clin Med. 2025. PMID: 39941629 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous