

CCL4 as a potential serum factor in differential diagnosis of central nervous system inflammatory diseases and gliomas
- PMID: 39364412
- PMCID: PMC11446780
- DOI: 10.3389/fimmu.2024.1461450
CCL4 as a potential serum factor in differential diagnosis of central nervous system inflammatory diseases and gliomas
Abstract
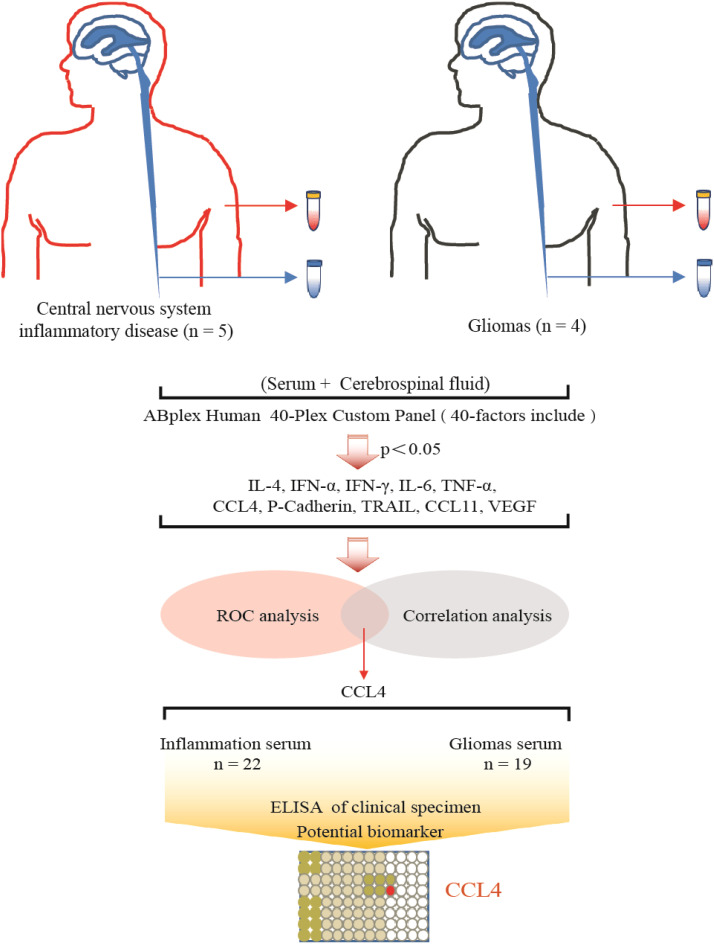
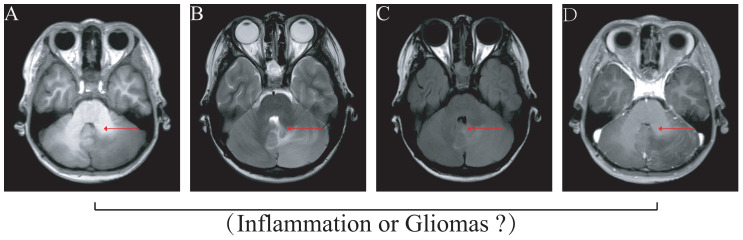
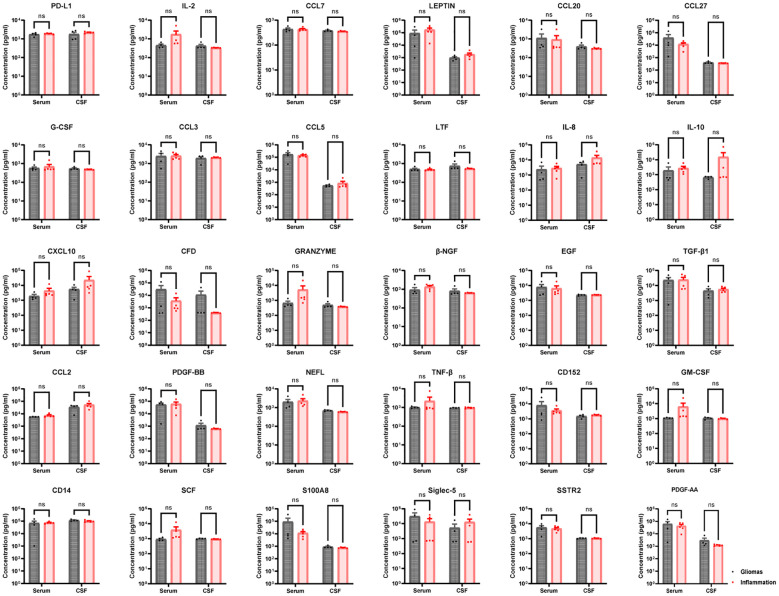
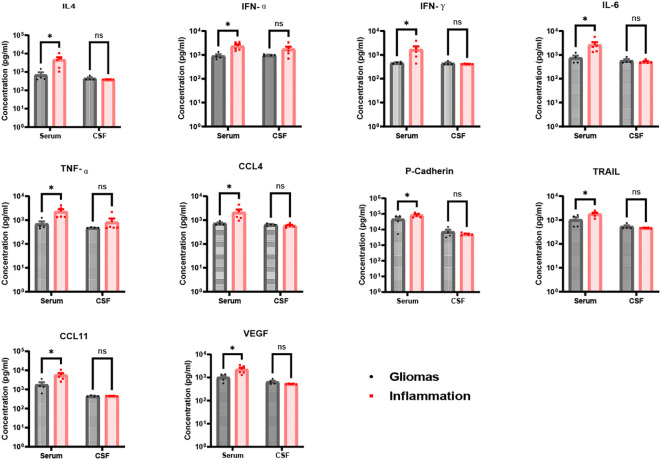
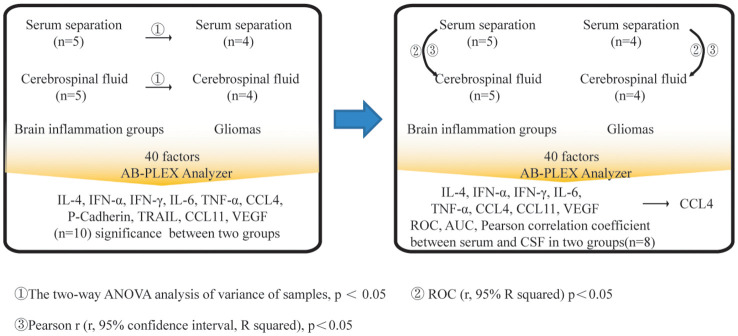
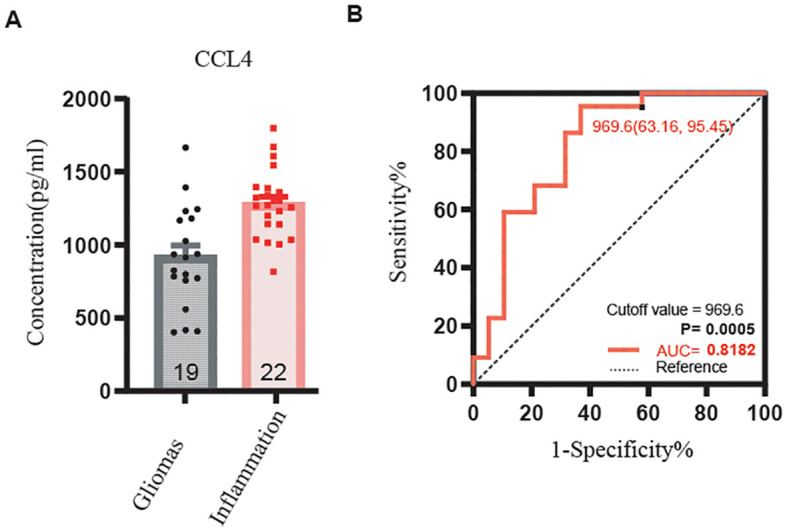
Computed tomography (CT) scans and magnetic resonance imaging (MRI) are commonly utilized to detect brain gliomas and central nervous system inflammation diseases. However, there are instances where depending solely on medical imaging for a precise diagnosis may result in unsuitable medications or treatments. Pathological analysis is regarded as the definitive method for diagnosing brain gliomas or central nervous system inflammation diseases. To achieve this, a craniotomy or stereotaxic biopsy is necessary to collect brain tissue, which can lead to complications such as cerebral hemorrhage, neurological deficits, cerebrospinal fluid leaks, and cerebral edema. Consequently, the advancement of non-invasive or minimally invasive diagnostic techniques is currently a high priority. This study included samples from four glioma patients and five patients with central nervous system inflammatory diseases, comprising both serum and paired cerebrospinal fluid (CSF). A total of 40 human cytokines were identified in these samples. We utilized a receiver operating characteristic (ROC) analysis to assess the sensitivity and specificity for distinguishing central nervous system inflammation diseases and gliomas. Additionally, we examined the correlation of these factors between serum and CSF in the patients. Ultimately, the identified factors were validated using serum from patients with clinically confirmed gliomas and central nervous system inflammation diseases followed by detection and statistical analysis through ELISA. The levels of serum factors IL-4, IFN-α, IFN-γ, IL-6, TNF-α, CCL4, CCL11, and VEGF were found to be significantly higher in gliomas compared with inflammatory diseases of the central nervous system (p < 0.05). Furthermore, a strong correlation was observed between the levels of CCL4 in serum and CSF, with a correlation coefficient of r = 0.92 (95% CI = 0.20-0.99, p = 0.027). We gathered more clinical samples to provide further validation of the abundance of CCL4 expression. A clinical study analyzing serum samples from 19 glioma patients and 22 patients with central nervous system inflammation diseases revealed that CCL4 levels were notably elevated in the inflammatory group compared with the glioma group (p < 0.001). These results suggest that assessing serum CCL4 levels may be useful in distinguishing those patients for clinical diagnostic purposes.
Keywords: central nervous system inflammatory diseases; clinical diagnosis; gliomas; non-invasive testing; non-invasive testing of biological structures; potential biomarker.
Copyright © 2024 Lyu, Wang, Zhao, Sun, Zhao, Tian, Guo, Wang, Zhao, Ma, Zhang and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer QC declared a shared affiliation, with no collaboration, with several of the authors, T-JL, ZZ, RT, HW, MZ, WX, to the handling editor at the time of the review.
Figures
Similar articles
-
Serum beta2-microglobulin acts as a biomarker for severity and prognosis in glioma patients: a preliminary clinical study.BMC Cancer. 2024 Jun 6;24(1):692. doi: 10.1186/s12885-024-12441-0. BMC Cancer. 2024. PMID: 38844902 Free PMC article.
-
The Role of Peripheral Inflammatory Markers and Coagulation Factors in Patients with Central Nervous System (CNS) Immune Disease and Glioma.World Neurosurg. 2024 Aug;188:e177-e193. doi: 10.1016/j.wneu.2024.05.080. Epub 2024 May 17. World Neurosurg. 2024. PMID: 38763458
-
A restricted signature of serum miRNAs distinguishes glioblastoma from lower grade gliomas.J Exp Clin Cancer Res. 2016 Jul 30;35(1):124. doi: 10.1186/s13046-016-0393-0. J Exp Clin Cancer Res. 2016. PMID: 27476114 Free PMC article.
-
Liquid biopsy and tumor DNA/RNA detection in the cerebrospinal fluid of patients diagnosed with central nervous system glioma - A review article.Surg Neurol Int. 2023 May 26;14:183. doi: 10.25259/SNI_52_2023. eCollection 2023. Surg Neurol Int. 2023. PMID: 37292399 Free PMC article. Review.
-
Multiple cerebral gliomas mimicking central nervous system inflammatory demyelinating diseases: A rare case with review of literature.Medicine (Baltimore). 2017 Dec;96(52):e9456. doi: 10.1097/MD.0000000000009456. Medicine (Baltimore). 2017. PMID: 29384930 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical