

A delayed presentation of traumatic diaphragmatic hernia in a young male: a unusual case report and comprehensive review of literature
- PMID: 39364427
- PMCID: PMC11445712
- DOI: 10.1093/jscr/rjae613
A delayed presentation of traumatic diaphragmatic hernia in a young male: a unusual case report and comprehensive review of literature
Abstract
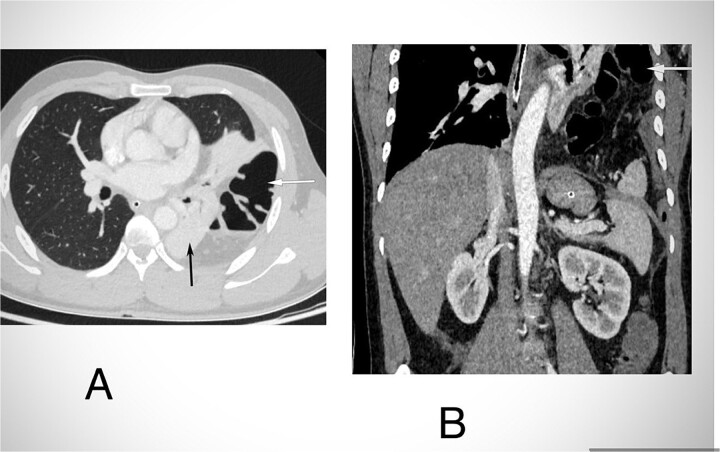
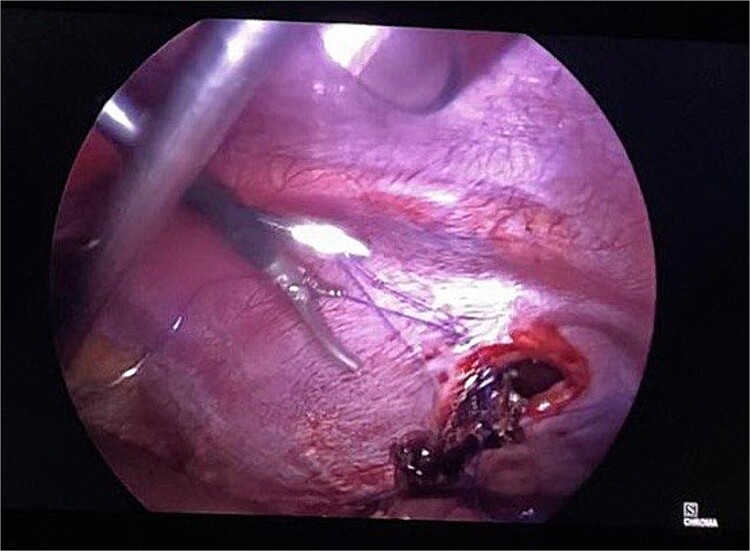
Acquired diaphragmatic hernia is typically caused by blunt trauma to the abdomen. It can be challenging to diagnose in acute cases due to a wide range of symptoms. Delayed presentation of traumatic diaphragmatic hernia is uncommon and can lead to respiratory issues or bowel complications like incarceration, perforation, or strangulation. Computed tomography is the preferred diagnostic tool. For acute case, laparotomy is indicated traditionally; however, the choice of surgery is dependent upon the surgeon's expertise and availability of resources.
Keywords: diaphragmatic hernia; incarceration; mesh; perforation.
Published by Oxford University Press and JSCR Publishing Ltd. © The Author(s) 2024.
Conflict of interest statement
None declared.
Figures




Similar articles
-
Delayed Presentation of Post-traumatic Multiorgan Left Diaphragmatic Hernia: A Case Report and Literature Review.Cureus. 2022 Jul 13;14(7):e26814. doi: 10.7759/cureus.26814. eCollection 2022 Jul. Cureus. 2022. PMID: 35971354 Free PMC article.
-
Post-traumatic diaphragmatic hernia: a rare case of intestinal obstruction.J Surg Case Rep. 2025 Mar 26;2025(3):rjaf163. doi: 10.1093/jscr/rjaf163. eCollection 2025 Mar. J Surg Case Rep. 2025. PMID: 40145011 Free PMC article.
-
Delayed presentation of a post-traumatic large right diaphragmatic hernia displacing liver and gallbladder - A case report.Asian J Endosc Surg. 2022 Apr;15(2):388-392. doi: 10.1111/ases.13015. Epub 2022 Feb 7. Asian J Endosc Surg. 2022. PMID: 35132800
-
Intrathoracic transverse colon and small bowel infarction in a patient with traumatic diaphragmatic hernia. Case report and review of the literature.J Med Liban. 2004 Jul-Sep;52(3):168-70. J Med Liban. 2004. PMID: 16432976 Review.
-
Acquired right-sided diaphragmatic hernia in a patient with retroperitoneal hydatidosis: a case report and review of the literature.J Med Case Rep. 2021 Jun 18;15(1):320. doi: 10.1186/s13256-021-02836-z. J Med Case Rep. 2021. PMID: 34140046 Free PMC article. Review.
Cited by
-
The Perception of the Diaphragm with Ultrasound: Always There Yet Overlooked?Life (Basel). 2025 Feb 5;15(2):239. doi: 10.3390/life15020239. Life (Basel). 2025. PMID: 40003648 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
