

Supplemental Screening as an Adjunct to Mammography for Breast Cancer Screening in People With Dense Breasts: A Health Technology Assessment
- PMID: 39364436
- PMCID: PMC11445669
Supplemental Screening as an Adjunct to Mammography for Breast Cancer Screening in People With Dense Breasts: A Health Technology Assessment
Abstract
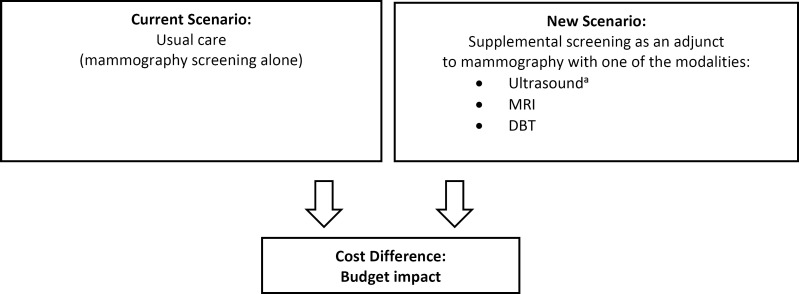
Background: Screening with mammography aims to detect breast cancer before clinical symptoms appear. Among people with dense breasts, some cancers may be missed using mammography alone. The addition of supplemental imaging as an adjunct to screening mammography has been suggested to detect breast cancers missed on mammography, potentially reducing the number of deaths associated with the disease. We conducted a health technology assessment of supplemental screening with contrast-enhanced mammography, ultrasound, digital breast tomosynthesis (DBT), or magnetic resonance imaging (MRI) as an adjunct to mammography for people with dense breasts, which included an evaluation of effectiveness, harms, cost-effectiveness, the budget impact of publicly funding supplemental screening, the preferences and values of patients and health care providers, and ethical issues.
Methods: We performed a systematic literature search of the clinical evidence published from January 2015 to October 2021. We assessed the risk of bias of each included study using the Cochrane Risk of Bias or RoBANS tools, and the quality of the body of evidence according to the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group criteria. We performed a systematic economic literature review and conducted cost-effectiveness analyses with a lifetime horizon from a public payer perspective. We also analyzed the budget impact of publicly funding supplemental screening as an adjunct to mammography for people with dense breasts in Ontario. To contextualize the potential value of supplemental screening for dense breasts, we spoke with people with dense breasts who had undergone supplemental screening; performed a rapid review of the qualitative literature; and conducted an ethical analysis of supplemental screening as an adjunct to mammography.
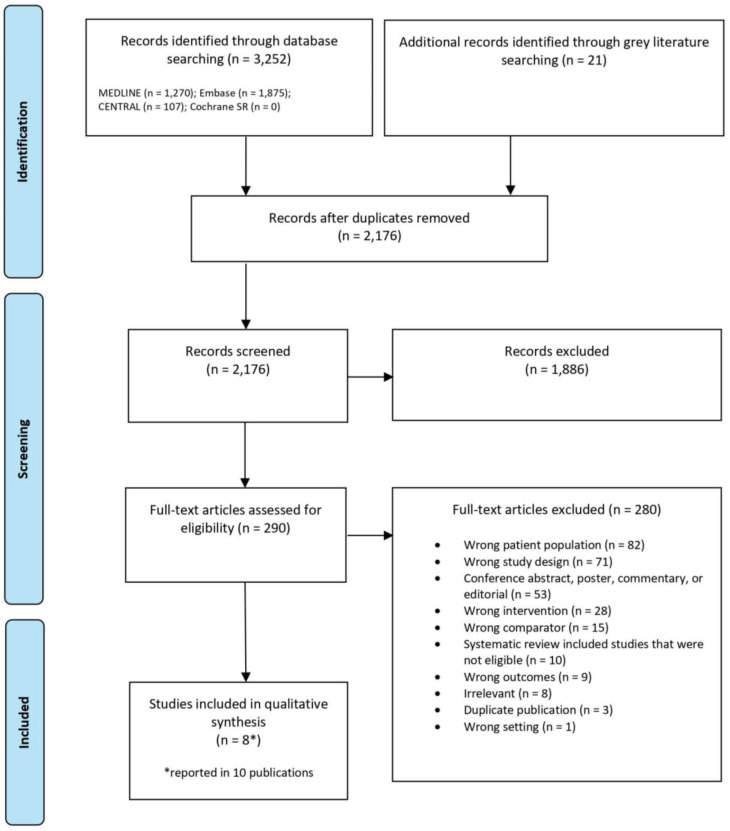
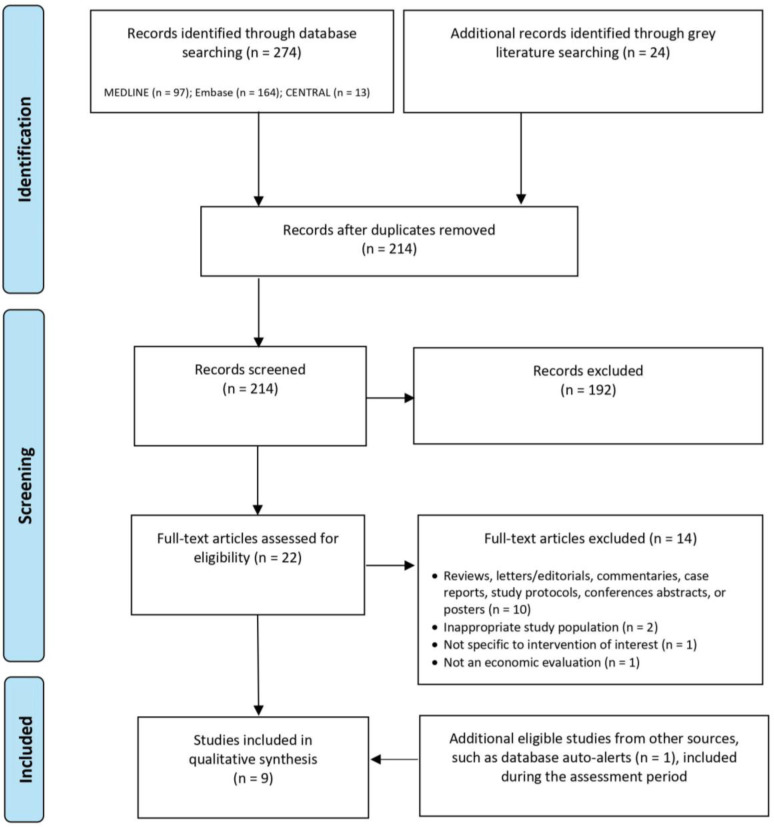
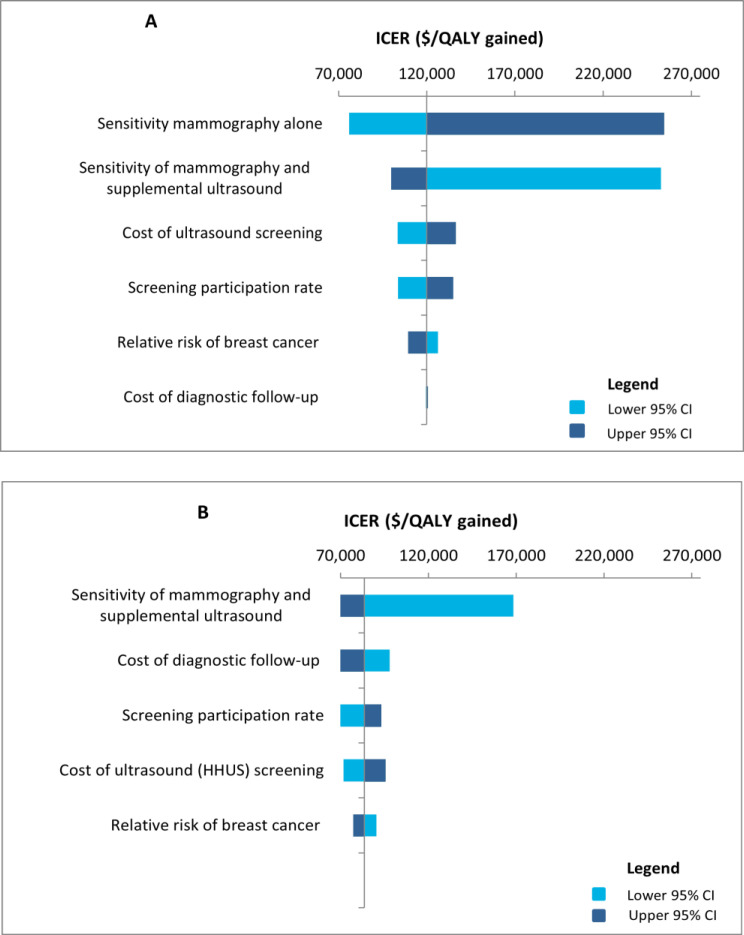
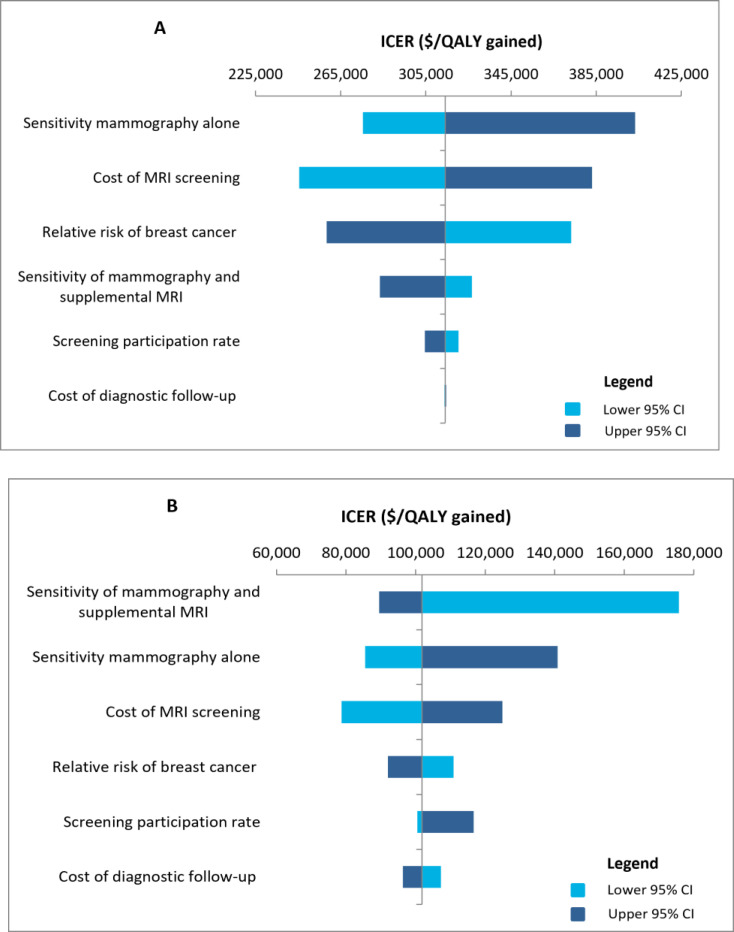
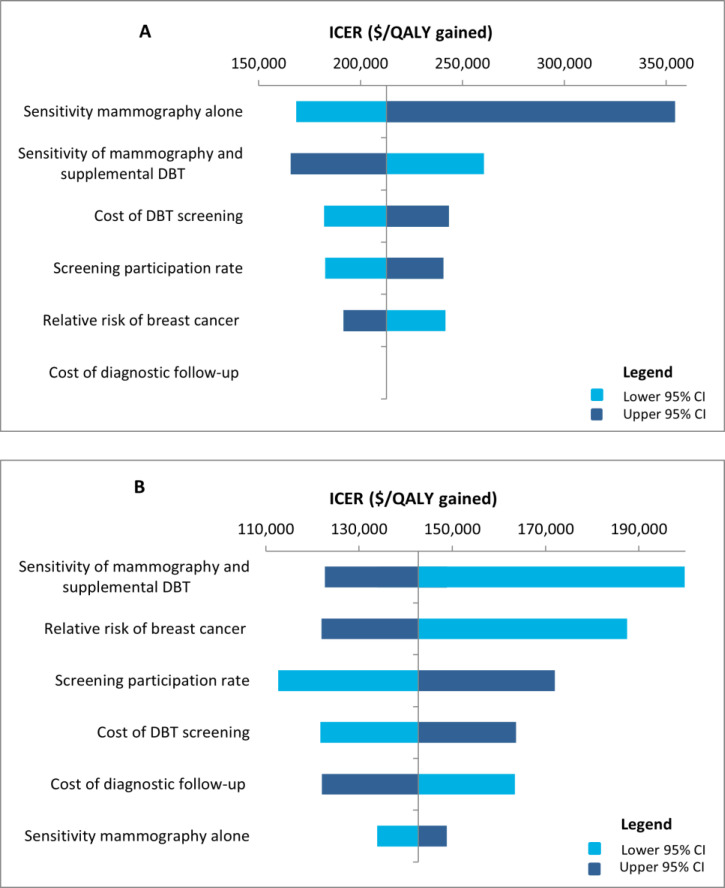
Results: We included eight primary studies in the clinical evidence review. No studies evaluated contrast-enhanced mammography. Nonrandomized and randomized evidence (GRADE: Very low to Moderate) suggests that mammography plus ultrasound was more sensitive and less specific, and detected more cancers compared to mammography alone. Fewer interval cancers occurred after mammography plus ultrasound (GRADE: Very low to Low), but recall rates were nearly double that of mammography alone (GRADE: Very low to Moderate). Evidence of Low to Very low quality suggested that compared with supplemental DBT, supplemental ultrasound was more sensitive, detected more cancers, and led to more recalls. Among people with extremely dense breasts, fewer interval cancers occurred after mammography plus supplemental MRI compared to mammography alone (GRADE: High). Supplemental MRI after negative mammography was highly accurate in people with extremely dense breasts and heterogeneously dense breasts in nonrandomized and randomized studies (GRADE: Very Low and Moderate). In people with extremely dense breasts, MRI after negative mammography detected 16.5 cancers per 1,000 screens (GRADE: Moderate), and up to 9.5% of all people screened were recalled (GRADE: Moderate). Contrast-related adverse events were infrequent (GRADE: Moderate). No study reported psychological impacts, breast cancer-specific mortality, or overall mortality.We included nine studies in the economic evidence, but none of the study findings was directly applicable to the Ontario context. Our lifetime cost-effectiveness analyses showed that supplemental screening with ultrasound, MRI, or DBT found more screen-detected cancers, decreased the number of interval cancers, had small gains in life-years or quality-adjusted life-years (QALYs), and was associated with savings in cancer management costs. However, supplemental screening also increased imaging costs and the number of false-positive cases. Compared to mammography alone, the incremental cost-effectiveness ratios (ICERs) for supplemental screening with handheld ultrasound, MRI, or DBT for people with dense breasts were $119,943, $314,170, and $212,707 per QALY gained, respectively. The ICERs for people with extremely dense breasts were $83,529, $101,813, and $142,730 per QALY gained, respectively. In sensitivity analyses, the diagnostic test sensitivity of mammography alone and of mammography plus supplemental screening had the greatest effect on ICER estimates. The total budget impact of publicly funding supplemental screening with handheld ultrasound, MRI, or DBT for people with dense breasts over the next 5 years is estimated at $15 million, $41 million, or $33 million, respectively. The corresponding total budget impact for people with extremely dense breasts is $4 million, $10 million, or $9 million.We engaged directly with 70 people via interviews and an online survey. The participants provided diverse perspectives on broad access to supplemental screening for people with dense breasts in Ontario. Themes discussed in the interviews included self-advocacy, patient-doctor partnership, preventive care, and a shared preference for broad access to screening modalities that are clinically effective in detecting breast cancer in people with dense breasts.We included 10 studies in the qualitative evidence rapid review. Thematic synthesis of these reports yielded three analytical themes: coming to know and understand breast density, which included introductions to and making sense of breast density; experiences of vulnerability, which influenced or were influenced by understandings and misunderstandings of breast density and responses to breast density; and choosing supplemental screening, which was influenced by knowledge and perception of the risks and benefits of supplemental screening, and the availability of resources.The ethics review determined that the main harms of supplemental screening for people with dense breasts are false-positives and overdiagnosis, both of which lead to unnecessary and burdensome health care treatments. Screening programs raise inherent tensions between individual- and population-level interests; they may yield population-level benefit, but are statistically of very little benefit to individuals. Entrenched cultural beliefs about the value of breast cancer screening, combined with uncertainty about the effects of supplemental screening on some outcomes and the discomfort of many health care providers in discussing screening options for people with dense breasts suggest that it may be difficult to ensure that patients can provide informed consent to engage in supplemental screening. Funding supplemental screening for people with dense breasts may lead to improved equity in the effectiveness of identifying cancers in people with dense breasts (compared to mammography alone), but it is not clear whether it would lead to equity in terms of improved survival and decreased morbidity.
Conclusions: Supplemental screening with ultrasound, DBT, or MRI as an adjunct to mammography detected more cancers and increased the number of recalls and biopsies, including false-positive results. Fewer interval cancers tended to occur after supplemental screening compared to mammography alone. It is unclear whether supplemental screening as an adjunct to mammography would reduce breast cancer-related or overall mortality among people with dense breasts.Supplemental screening with ultrasound, DBT, or MRI as an adjunct to mammography in people aged 50 to 74 years improved cancer detection but increased costs. Depending on the type of imaging modality, publicly funding supplemental screening in Ontario over the next 5 years would require additional total costs between $15 million and $41 million for people with dense breasts, and between $4 million and $10 million for people with extremely dense breasts.The people we engaged with directly valued the potential clinical benefits of supplemental screening and emphasized that patient education and equitable access should be a requirement for implementation in Ontario. Our review of the qualitative literature found that the concept of breast density is poorly understood, both by people with dense breasts and by some general practitioners. People with dense breasts who receive routine mammography (especially those who receive health care in their nonpreferred language or are perceived to have lower economic status or health literacy) and their general practitioners may not have the awareness or knowledge to make informed decisions about supplemental screening. Some people with dense breasts experienced emotional distress from barriers to accessing supplemental screening, and many wanted to engage in supplemental screening, even when educated about its potential harms, including false-positives and overdiagnosis.Given an overall lack of robust evidence about morbidity and mortality associated with supplemental screening for people with dense breasts, it is not possible to determine whether funding supplemental screening for dense breasts delivers on the ethical duties to maximize benefits and minimize harms for populations and individuals. It is likely that existing inequities in access to breast screening and cancer treatment will persist, even if supplemental screening for dense breasts is funded. Continued efforts to address these inequities by removing barriers to screening might mitigate this concern. It will be important to identify and minimize sources of uncertainty related to benefits and risks of supplemental screening for dense breasts to optimize the capacity for everyone involved to live up to their ethical obligations. Some of these may be resolved with further evidence related to the outcomes of supplemental screening for dense breasts.
Copyright © King's Printer for Ontario, 2023.
Figures

Similar articles
-
Digital Breast Tomosynthesis with Hologic 3D Mammography Selenia Dimensions System for Use in Breast Cancer Screening: A Single Technology Assessment [Internet].Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Sep 4. Report from the Norwegian Institute of Public Health No. 2017-08. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Sep 4. Report from the Norwegian Institute of Public Health No. 2017-08. PMID: 29553669 Free Books & Documents. Review.
-
Supplemental Screening for Breast Cancer in Women With Dense Breasts: A Systematic Review for the U.S. Preventive Service Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Jan. Report No.: 14-05201-EF-3. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Jan. Report No.: 14-05201-EF-3. PMID: 26866210 Free Books & Documents. Review.
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
Carrier Screening Programs for Cystic Fibrosis, Fragile X Syndrome, Hemoglobinopathies and Thalassemia, and Spinal Muscular Atrophy: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Aug 10;23(4):1-398. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 37637488 Free PMC article.
-
Homologous Recombination Deficiency Testing to Inform Patient Decisions About Niraparib Maintenance Therapy for High-Grade Serous or Endometrioid Epithelial Ovarian Cancer: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Aug 10;23(5):1-188. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 37637244 Free PMC article.
Cited by
-
Meta-analysis of the synergistic effect of magnetic resonance imaging and mammography in breast cancer detection in women with dense breasts.Am J Transl Res. 2025 Mar 15;17(3):1554-1567. doi: 10.62347/BMWY7899. eCollection 2025. Am J Transl Res. 2025. PMID: 40226002 Free PMC article. Review.
-
Effect of Breast Screening Regimen on Breast Cancer Outcomes: A Modeling Study.Curr Oncol. 2023 Oct 25;30(11):9475-9483. doi: 10.3390/curroncol30110686. Curr Oncol. 2023. PMID: 37999106 Free PMC article.
-
Breast density notification: Are family doctors prepared to counsel patients on risks and management?Can Fam Physician. 2023 Nov;69(11):748-750. doi: 10.46747/cfp.6911748. Can Fam Physician. 2023. PMID: 37963789 Free PMC article. No abstract available.
-
Added Value of a Previous Exam Comparison in the Final Breast Imaging and Reporting Data System (BI-RADS®) Assessment in Screening Mammography.Cureus. 2024 Oct 29;16(10):e72616. doi: 10.7759/cureus.72616. eCollection 2024 Oct. Cureus. 2024. PMID: 39618601 Free PMC article.
References
-
- Breast cancer statistics [Internet]. Toronto (ON): Canadian Cancer Society; c2021. [cited 2021 Jul 12]. Available from: www.cancer.ca/en/cancer-information/cancer-type/breast/statistics/?regio...
-
- Canadian Partnership Against Cancer. Breast cancer control in Canada: a system performance special focus report. Toronto (ON): Canadian Partnership Against Cancer; 2012.
-
- SEER cancer statistics review, 1975–2017 [Internet]. Bethesda (MD): National Cancer Institute; 2020. [cited 2022 Dec 19]. Available from: https://seer.cancer.gov/csr/1975_2017
-
- Types of cancer: breast cancer [Internet]. Toronto (ON): Cancer Care Ontario; [cited 2021 May 22]. Available from: www.cancercareontario.ca/en/types-of-cancer/breast-cancer
-
- PDQ Screening and Prevention Editorial Board. PDQ Screening and Prevention Editorial Board: National Cancer Institute; 2021. [cited 2021 May 26]. Available from: www.cancer.gov/types/breast/hp/breast-screening-pdq
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical