

Giant Primary Cutaneous Myoepithelial Carcinoma of the Left Thigh With Inguinal and Pelvic Lymph Node Metastases
- PMID: 39364518
- PMCID: PMC11449504
- DOI: 10.7759/cureus.68571
Giant Primary Cutaneous Myoepithelial Carcinoma of the Left Thigh With Inguinal and Pelvic Lymph Node Metastases
Abstract
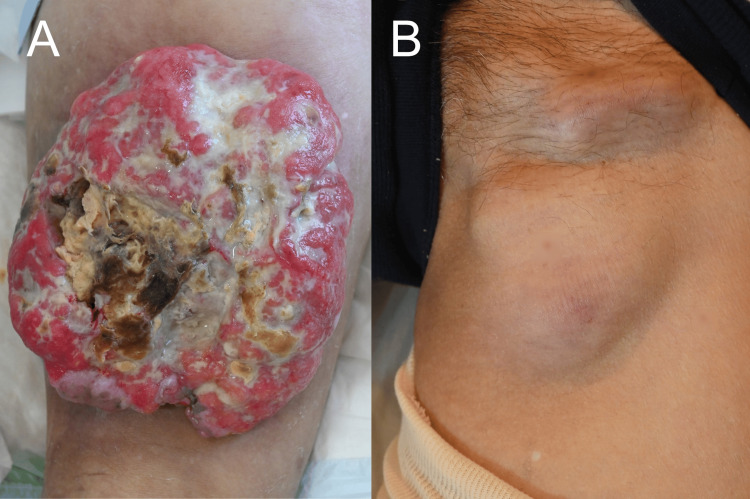
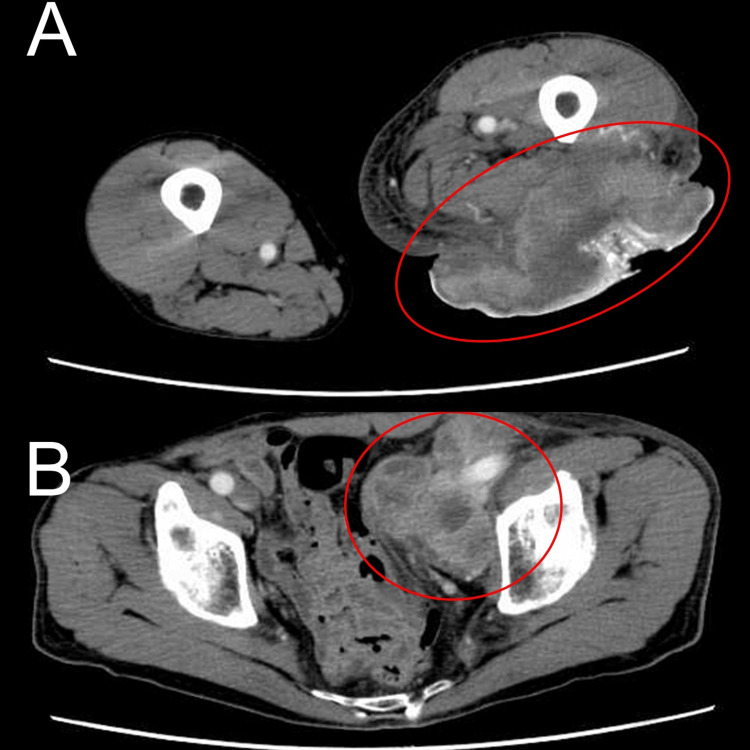
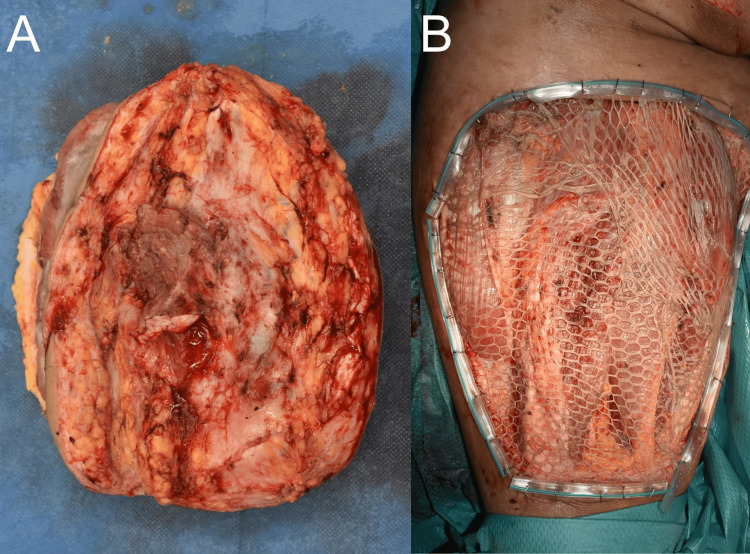
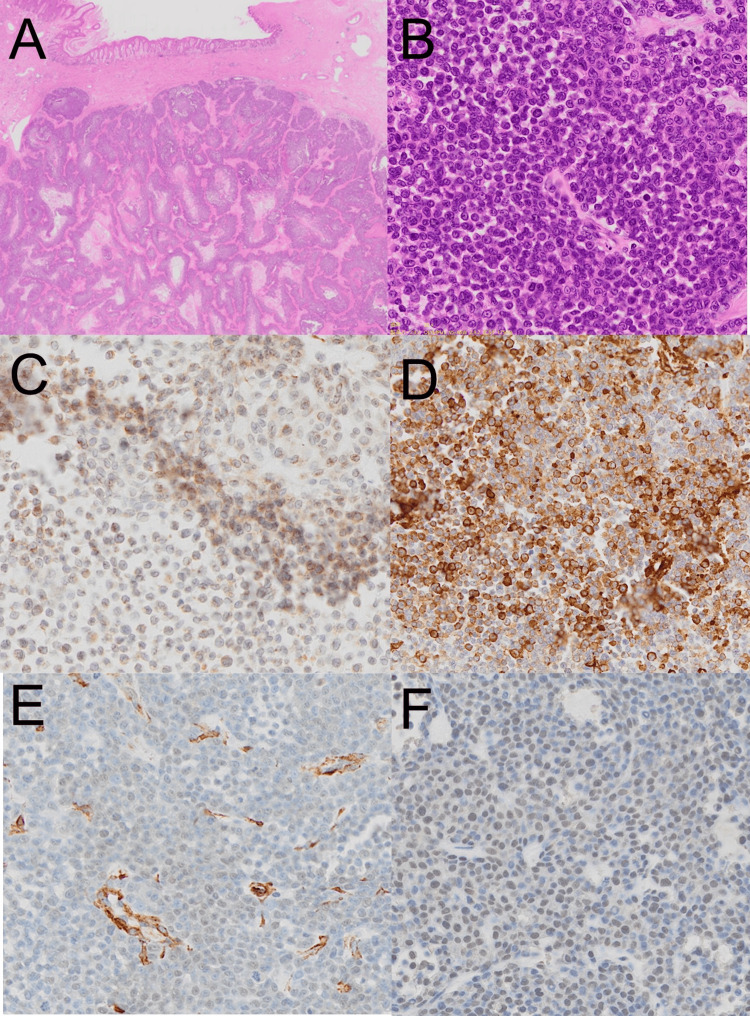
Myoepithelial carcinoma is an exceedingly rare malignancy, particularly when originating from the skin. It frequently arises from malignant transformations of pleomorphic adenomas in various locations such as the parotid gland, breast, soft tissues, and lungs. Primary cutaneous myoepithelial carcinoma is exceptionally rare, often leading to delayed diagnosis. We report a case of giant primary cutaneous myoepithelial carcinoma of the left thigh, initially misdiagnosed as squamous cell carcinoma (SCC). The patient, a 64-year-old male, presented with a rapidly enlarging, ulcerated, and necrotic skin lesion. The initial presentation mimicked SCC. Due to the large tumor size and anemia caused by the tumor, the patient underwent a reduced-dose chemotherapy regimen (cytarabine plus aclarubicin chemotherapy) to shrink the tumor, enabling successful local surgical resection. Post-surgery, the patient received radiotherapy and tegafur gimeracil oteracil potassium, resulting in disease control without progression for two years. This case highlights the diagnostic challenges of myoepithelial carcinoma, which can mimic SCC among numerous other tumors. Accurate diagnosis relies on immunohistochemical staining and careful pathological evaluation. The case underscores the importance of considering myoepithelial carcinoma in the differential diagnosis of ulcerative tumors.
Keywords: case report; chemotherapy; myoepithelial carcinoma; skin cancer; surgical resection.
Copyright © 2024, Obata et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Primary cutaneous myoepithelial carcinoma: a case report and review of the literature. Frost MW, Steiniche T, Damsgaard TE, Stolle LB. APMIS. 2014;122:369–379. - PubMed
-
- Cutaneous myoepithelial carcinoma with disseminated metastases. Johnson GE, Stevens K, Morrison AO, Stuart L, Gardner JM, Rachal M, Parker DC. https://www.mdedge.com/dermatology/article/140924/nonmelanoma-skin-cance... Cutis. 2017;99:19. - PubMed
-
- A case of cutaneous myoepithelial carcinoma. Tanahashi J, Kashima K, Daa T, Kondo Y, Kuratomi E, Yokoyama S. J Cutan Pathol. 2007;34:648–653. - PubMed
-
- Association between prognosis and complete resection in primary cutaneous myoepithelial carcinoma: two case presentations and literature review. Mizuta H, Takahashi A, Namikawa K, Ogata D, Yamazaki N. Dermatol Ther. 2020;33:0. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials