

Multipoint pacing is associated with improved prognosis and cardiac resynchronization therapy response: MORE-CRT MPP randomized study secondary analyses
- PMID: 39365705
- PMCID: PMC11572720
- DOI: 10.1093/europace/euae259
Multipoint pacing is associated with improved prognosis and cardiac resynchronization therapy response: MORE-CRT MPP randomized study secondary analyses
Erratum in
-
Correction to: Multipoint pacing is associated with improved prognosis and cardiac resynchronization therapy response: MORE-CRT MPP randomized study secondary analyses.Europace. 2025 Feb 5;27(2):euaf022. doi: 10.1093/europace/euaf022. Europace. 2025. PMID: 39964068 Free PMC article. No abstract available.
Abstract
Aims: Cardiac resynchronization therapy (CRT) via biventricular (BIV) pacing is indicated in patients with heart failure (HF), reduced ejection fraction, and prolonged QRS duration. Quadripolar leads and multipoint pacing (MPP) allow multiple left ventricle (LV) sites pacing. We aimed to assess the clinical benefit of MPP in patients who do not respond to standard BIV pacing.
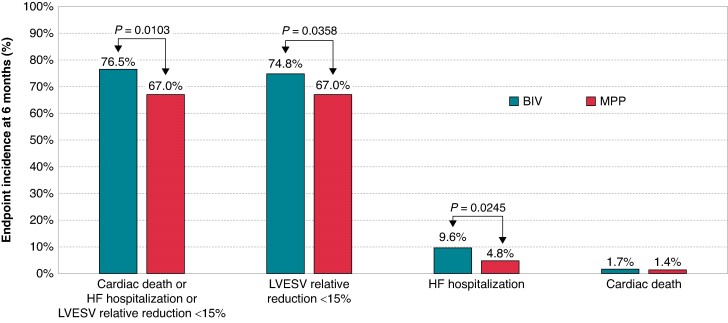
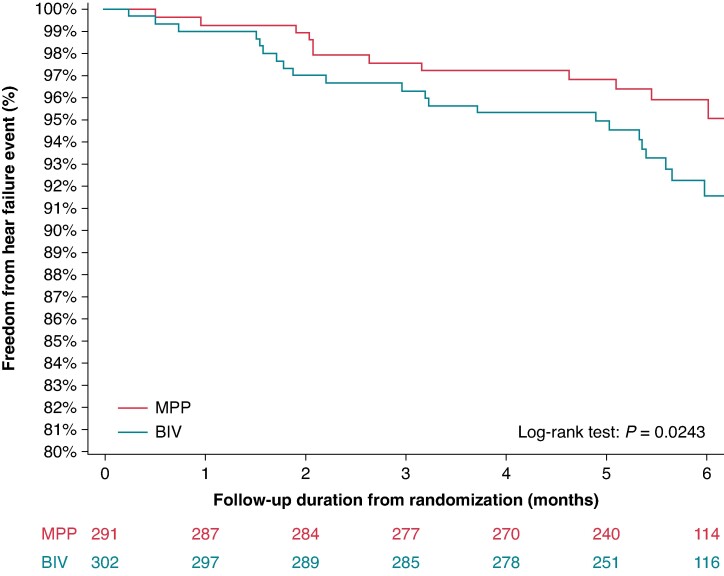
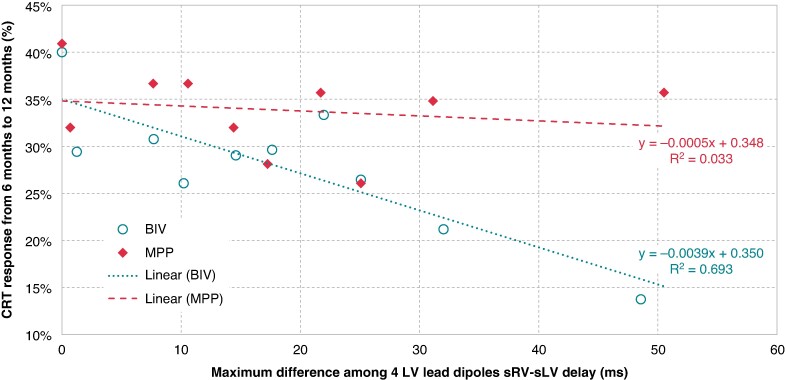
Methods and results: Overall, 3724 patients were treated with standard BIV pacing. After 6 months, 1639 patients were considered as CRT non-responders (echo-measured relative reduction in LV end-systolic volume (LVESV) < 15%) and randomized to MPP or BIV. We analysed 593 randomized patients (291 MPP, 302 BIV), who had BIV pacing >97% of the time before randomization and complete 12 months of clinical and echocardiographic data. The endpoint composed of freedom from cardiac death and HF hospitalizations and by LVESV relative reduction ≥15% between randomization and 12 months occurred more frequently in MPP [96/291 (33.0%)] vs. BIV [71/302 (23.5%), P = 0.0103], which was also confirmed at multivariate analysis (hazard ratio = 1.55, 95% confidence interval = 1.02-2.34, P = 0.0402 vs. BIV). HF hospitalizations occurred less frequently in MPP [14/291 (4.81%)] vs. BIV [29/302 (9.60%), incidence rate ratio = 50%, P = 0.0245]. Selecting patients with a large (>30 ms) dispersion of interventricular electrical delay among the four LV lead dipoles, reverse remodelling was more frequent in MPP [18/51 (35.3%)] vs. BIV [11/62 (17.7%), P = 0.0335].
Conclusion: In patients who do not respond to standard CRT despite the high BIV pacing percentage, MPP is associated with lower occurrence of HF hospitalizations and higher probability of reverse LV remodelling compared with BIV pacing.
Keywords: Biventricular pacing; Cardiac resynchronization; Heart failure; MPP; Multipoint pacing; Quadripolar left ventricular pacing; Randomized controlled study.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Dr Rinaldi has received research funding and/or consultation fees from Abbott, Medtronic, Boston Scientific, Spectranetics, EBR Systems, and MicroPort outside of the submitted work. Dr Leclercq has received honoraria from Abbott, Medtronic, Boston Scientific, Biotronik, and Livanova. Dr Burri has received institutional fellowship support and research grants from Abbott. Dr Sperzel serves as a consultant to Abbott, in addition to receiving honoraria and currently conducting research sponsored by Abbott. Dr Thibault has received research support and honoraria from Abbott and Medtronic. Dr Lee, Ms Lin. and Mr Grammatico are employees of Abbott. All remaining authors have declared no conflicts of interest.
Figures


References
-
- Abraham WT. Cardiac resynchronization therapy for heart failure: biventricular pacing and beyond. Curr Opin Cardiol 2002;17:346–52. - PubMed
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IMet al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Developed by the Task Force on Cardiac Pacing and Cardiac Resynchronization Therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Europace 2022;24:71–164. - PubMed
-
- Forleo GB, Della Rocca DG, Papavasileiou LP, Molfetta AD, Santini L, Romeo F. Left ventricular pacing with a new quadripolar transvenous lead for CRT: early results of a prospective comparison with conventional implant outcomes. Heart Rhythm 2011;8:31–7. - PubMed
-
- Gutleben KJ, Kranig W, Barr C, Morgenstern MM, Simon M, Lee K. Multisite left ventricular pacing is safe and improves cardiac hemodynamic in heart failure patients—results from a 1-month follow-up study. Heart Rhythm 2013;5:S134–68.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
