

Toripalimab in combination with HBM4003, an anti-CTLA-4 heavy chain-only antibody, in advanced melanoma and other solid tumors: an open-label phase I trial
- PMID: 39366752
- PMCID: PMC11459314
- DOI: 10.1136/jitc-2024-009662
Toripalimab in combination with HBM4003, an anti-CTLA-4 heavy chain-only antibody, in advanced melanoma and other solid tumors: an open-label phase I trial
Abstract
Background: HBM4003 is a novel anti-CTLA-4 heavy chain-only antibody, designed to enhance Treg ablation and antibody-dependent cell-mediated cytotoxicity while ensuring a manageable safety profile. This phase I trial investigated the safety, pharmacokinetics, immunogenicity and preliminary efficacy of HBM4003 plus with anti-PD-1 antibody toripalimab in patients with advanced solid tumors, especially focusing on melanoma.
Methods: The multicenter, open-label phase I trial was divided into two parts: dose-escalation phase (part 1) and dose-expansion phase (part 2). In part 1, HBM4003 was administered at doses of 0.03, 0.1, 0.3 mg/kg in combination with toripalimab with fixed dosage of 240 mg every 3 weeks. The recommended phase II dose (RP2D) was used in the expansion phase. Primary endpoints were safety and RP2D in part 1 and objective response rate (ORR) in part 2. Biomarkers based on cytokines and multiplex immunofluorescence staining were explored.
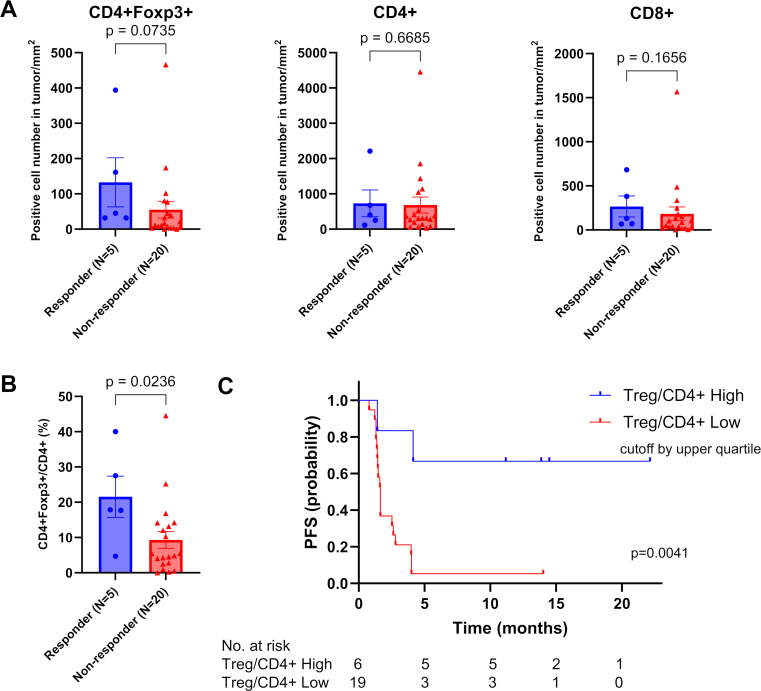
Results: A total of 40 patients received study treatment, including 36 patients treated with RP2D of HBM4003 0.3 mg/kg plus toripalimab 240 mg every 3 week. 36 participants (90.0%) experienced at least one treatment-related adverse event (TRAE), of which 10 (25.0%) patients experienced grade ≥3 TRAEs and 5 (12.5%) experienced immune-mediated adverse events (irAEs) with maximum severity of grade 3. No grade 4 or 5 irAEs occurred. Efficacy analysis set included 32 melanoma patients treated with RP2D and with available post-baseline imaging data. The ORRs of anti-PD-1/PD-L1 treatment-naïve subgroup and anti-PD-1/PD-L1 treatment-failed subgroup were 33.3% and 5.9%, respectively. In mucosal melanoma, the ORR of the two subgroups were 40.0% and 10.0%, respectively. Baseline high Treg/CD4+ratio in the tumor serves as an independent predictive factor for the efficacy of immunotherapy.
Conclusions: HBM4003 0.3 mg/kg plus toripalimab 240 mg every 3 week demonstrated manageable safety in solid tumors and no new safety signal. Limited data demonstrated promising antitumor activity, especially in PD-1 treatment-naïve mucosal melanoma.
Trial registration number: NCT04727164.
Keywords: Immunotherapy; Pharmacokinetics - PK; Solid tumor.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JG is a member of the advisory board/consultant of MSD, Roche, Pfizer, Bayer, Novartis, Simcere, Shanghai Junshi Bioscience, Oriengene.
Figures



Similar articles
-
Anti-LAG-3 antibody LBL-007 plus anti-PD-1 antibody toripalimab in advanced nasopharyngeal carcinoma and other solid tumors: an open-label, multicenter, phase Ib/II trial.J Hematol Oncol. 2025 Feb 7;18(1):15. doi: 10.1186/s13045-025-01666-6. J Hematol Oncol. 2025. PMID: 39920751 Free PMC article. Clinical Trial.
-
Dual CTLA-4 and PD-1 checkpoint blockade using CS1002 and CS1003 (nofazinlimab) in patients with advanced solid tumors: A first-in-human, dose-escalation, and dose-expansion study.Cancer. 2024 Jun 1;130(11):1991-2002. doi: 10.1002/cncr.35226. Epub 2024 Feb 26. Cancer. 2024. PMID: 38404184 Clinical Trial.
-
Axitinib in Combination With Toripalimab, a Humanized Immunoglobulin G4 Monoclonal Antibody Against Programmed Cell Death-1, in Patients With Metastatic Mucosal Melanoma: An Open-Label Phase IB Trial.J Clin Oncol. 2019 Nov 10;37(32):2987-2999. doi: 10.1200/JCO.19.00210. Epub 2019 Aug 12. J Clin Oncol. 2019. PMID: 31403867 Free PMC article. Clinical Trial.
-
Systematic review and meta-analysis efficacy and safety of immune checkpoint inhibitors in advanced melanoma patients with anti-PD-1 progression: a systematic review and meta-analysis.Clin Transl Oncol. 2021 Sep;23(9):1885-1904. doi: 10.1007/s12094-021-02598-6. Epub 2021 Apr 20. Clin Transl Oncol. 2021. PMID: 33877531
-
Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2020 Dec 14;12(12):CD013257. doi: 10.1002/14651858.CD013257.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 30;4:CD013257. doi: 10.1002/14651858.CD013257.pub3. PMID: 33316104 Free PMC article. Updated.
Cited by
-
Multicenter phase 1/2 study of onatasertib, a dual TORC1/2 inhibitor, combined with the PD-1 antibody toripalimab in advanced solid tumors.Signal Transduct Target Ther. 2025 Jun 25;10(1):198. doi: 10.1038/s41392-025-02281-0. Signal Transduct Target Ther. 2025. PMID: 40555721 Free PMC article. Clinical Trial.
-
Efficacy and safety of HBM4003 combined with toripalimab in refractory neuroendocrine neoplasms: a multicenter, phase II study.EClinicalMedicine. 2025 Jun 3;84:103249. doi: 10.1016/j.eclinm.2025.103249. eCollection 2025 Jun. EClinicalMedicine. 2025. PMID: 40521168 Free PMC article.
-
Application of Immune Checkpoint Inhibitors in Cancer.MedComm (2020). 2025 Aug 10;6(8):e70176. doi: 10.1002/mco2.70176. eCollection 2025 Aug. MedComm (2020). 2025. PMID: 40787068 Free PMC article. Review.
-
Advances in cancer immunotherapy: historical perspectives, current developments, and future directions.Mol Cancer. 2025 May 7;24(1):136. doi: 10.1186/s12943-025-02305-x. Mol Cancer. 2025. PMID: 40336045 Free PMC article. Review.
-
A novel model for predicting immunotherapy response and prognosis in NSCLC patients.Cancer Cell Int. 2025 May 15;25(1):178. doi: 10.1186/s12935-025-03800-3. Cancer Cell Int. 2025. PMID: 40375214 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials