

Artificial intelligence in commercial fracture detection products: a systematic review and meta-analysis of diagnostic test accuracy
- PMID: 39367147
- PMCID: PMC11452402
- DOI: 10.1038/s41598-024-73058-8
Artificial intelligence in commercial fracture detection products: a systematic review and meta-analysis of diagnostic test accuracy
Abstract
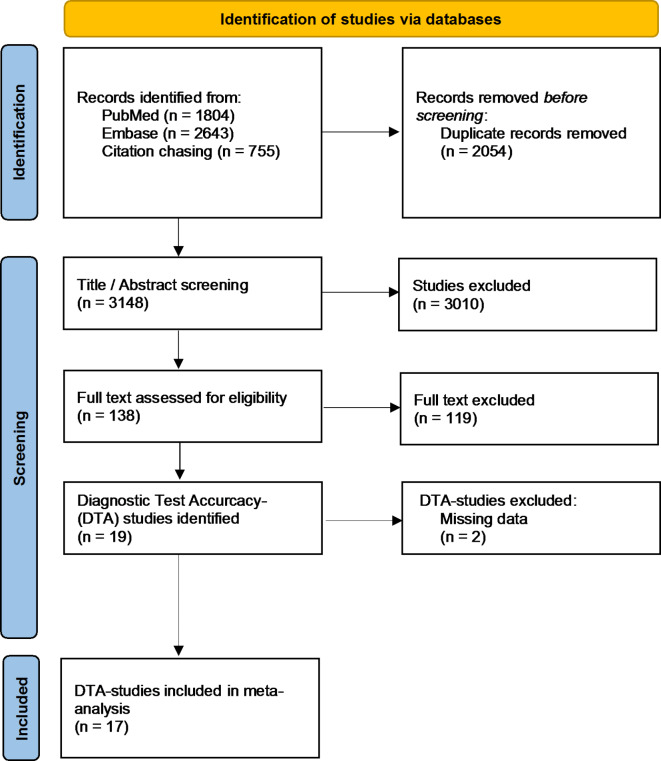
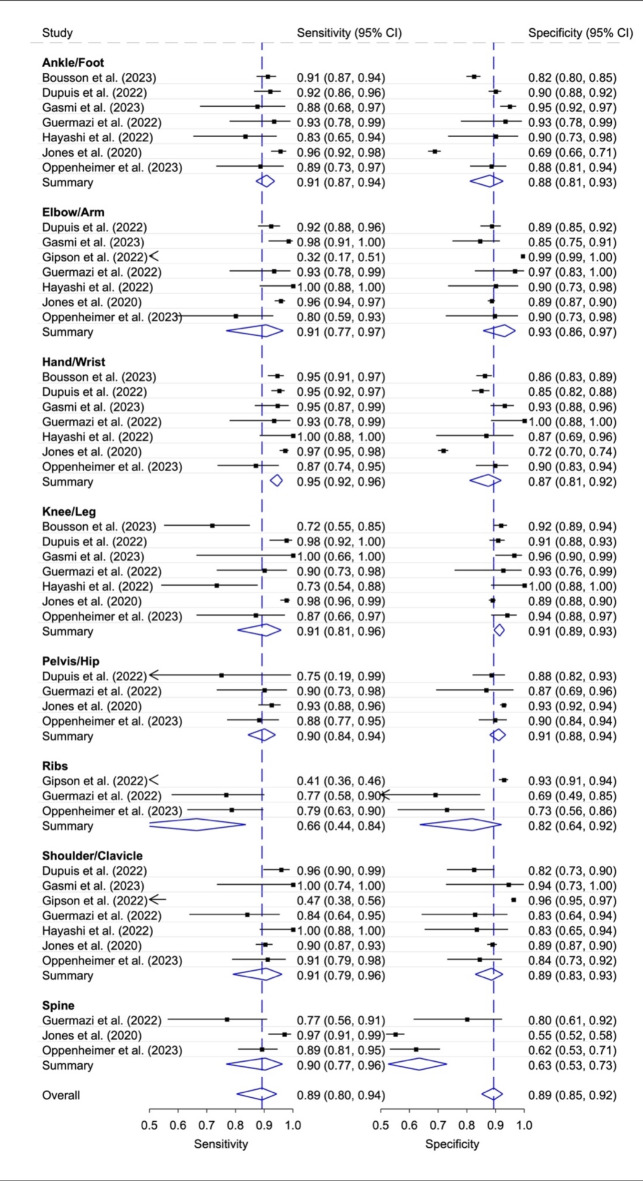
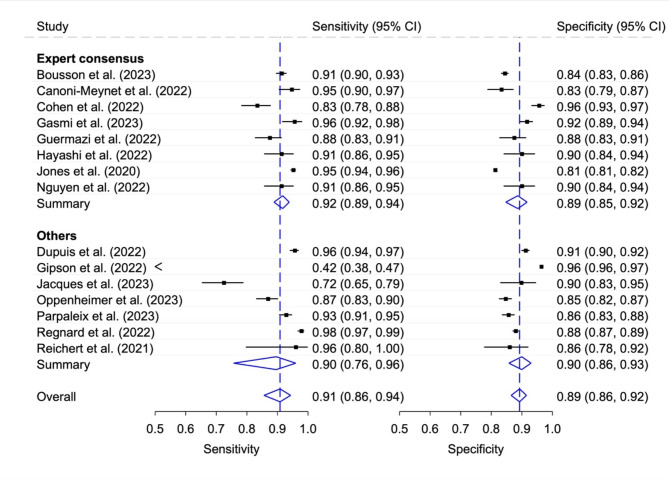
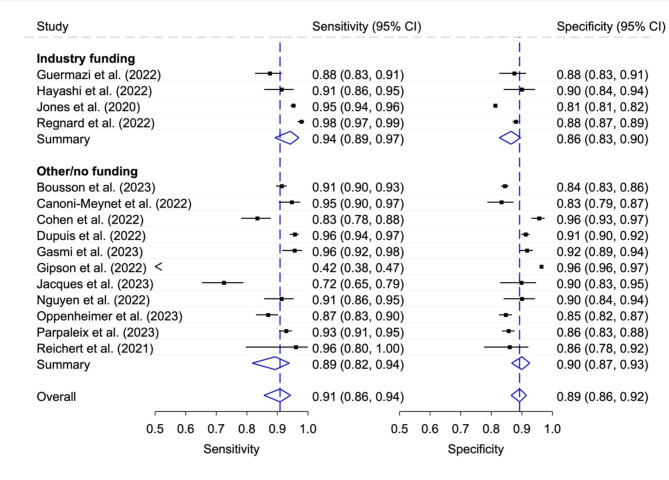
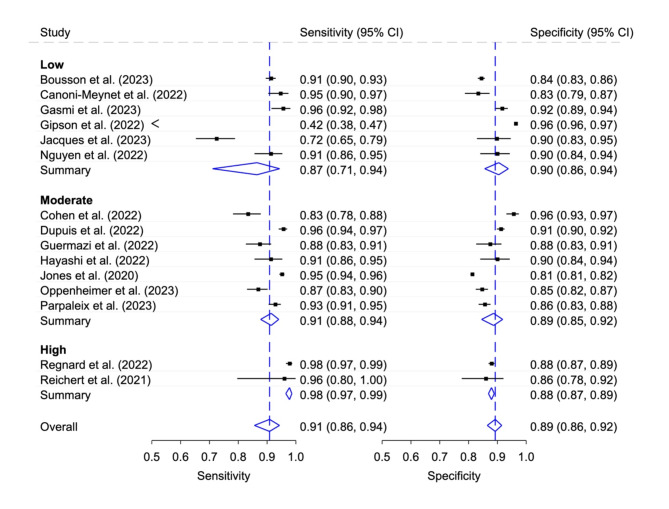
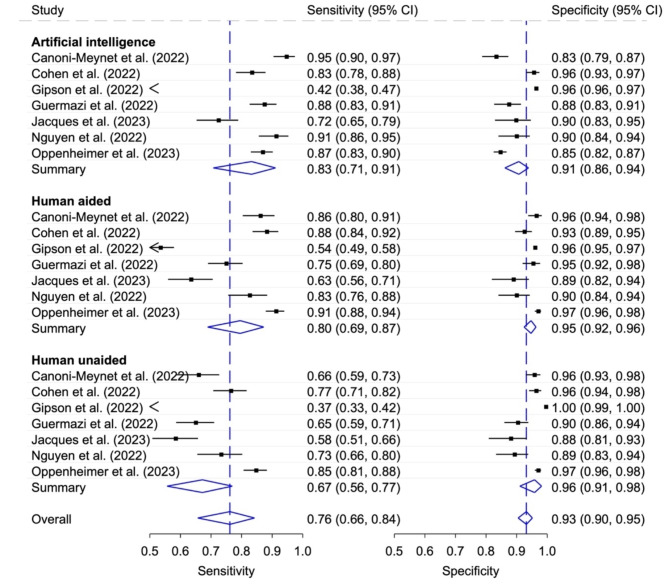
Conventional radiography (CR) is primarily utilized for fracture diagnosis. Artificial intelligence (AI) for CR is a rapidly growing field aimed at enhancing efficiency and increasing diagnostic accuracy. However, the diagnostic performance of commercially available AI fracture detection solutions (CAAI-FDS) for CR in various anatomical regions, their synergy with human assessment, as well as the influence of industry funding on reported accuracy are unknown. Peer-reviewed diagnostic test accuracy (DTA) studies were identified through a systematic review on Pubmed and Embase. Diagnostic performance measures were extracted especially for different subgroups such as product, type of rater (stand-alone AI, human unaided, human aided), funding, and anatomical region. Pooled measures were obtained with a bivariate random effects model. The impact of rater was evaluated with comparative meta-analysis. Seventeen DTA studies of seven CAAI-FDS analyzing 38,978 x-rays with 8,150 fractures were included. Stand-alone AI studies (n = 15) evaluated five CAAI-FDS; four with good sensitivities (> 90%) and moderate specificities (80-90%) and one with very poor sensitivity (< 60%) and excellent specificity (> 95%). Pooled sensitivities were good to excellent, and specificities were moderate to good in all anatomical regions (n = 7) apart from ribs (n = 4; poor sensitivity / moderate specificity) and spine (n = 4; excellent sensitivity / poor specificity). Funded studies (n = 4) had higher sensitivity (+ 5%) and lower specificity (-4%) than non-funded studies (n = 11). Sensitivity did not differ significantly between stand-alone AI and human AI aided ratings (p = 0.316) but specificity was significantly higher the latter group (p < 0.001). Sensitivity was significant lower in human unaided compared to human AI aided respectively stand-alone AI ratings (both p ≤ 0.001); specificity was higher in human unaided ratings compared to stand-alone AI (p < 0.001) and showed no significant differences AI aided ratings (p = 0.316). The study demonstrates good diagnostic accuracy across most CAAI-FDS and anatomical regions, with the highest performance achieved when used in conjunction with human assessment. Diagnostic accuracy appears lower for spine and rib fractures. The impact of industry funding on reported performance is small.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Burge, R. et al. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J. Bone Miner. Res.22, 465–475 (2007). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
