

Signaling pathways involved in colorectal cancer: pathogenesis and targeted therapy
- PMID: 39370455
- PMCID: PMC11456611
- DOI: 10.1038/s41392-024-01953-7
Signaling pathways involved in colorectal cancer: pathogenesis and targeted therapy
Abstract
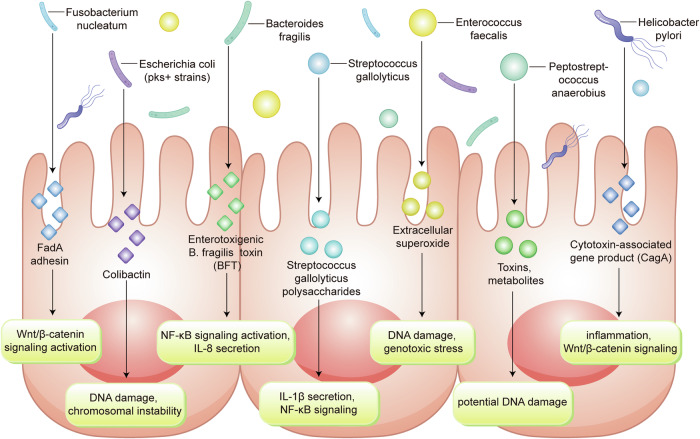
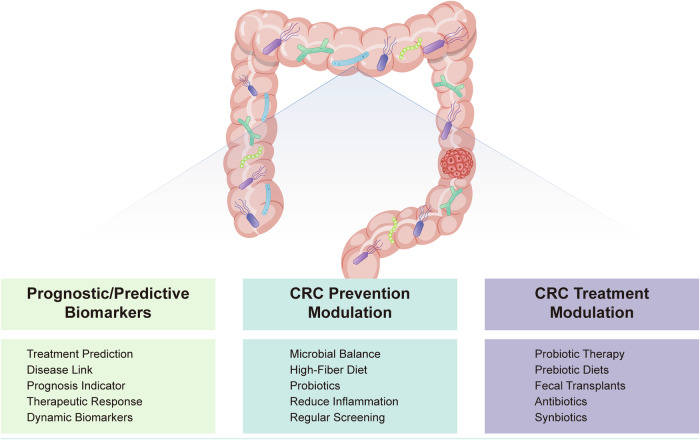
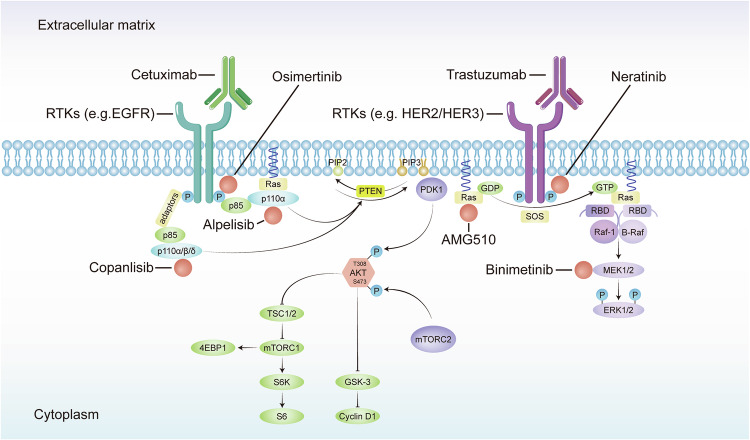
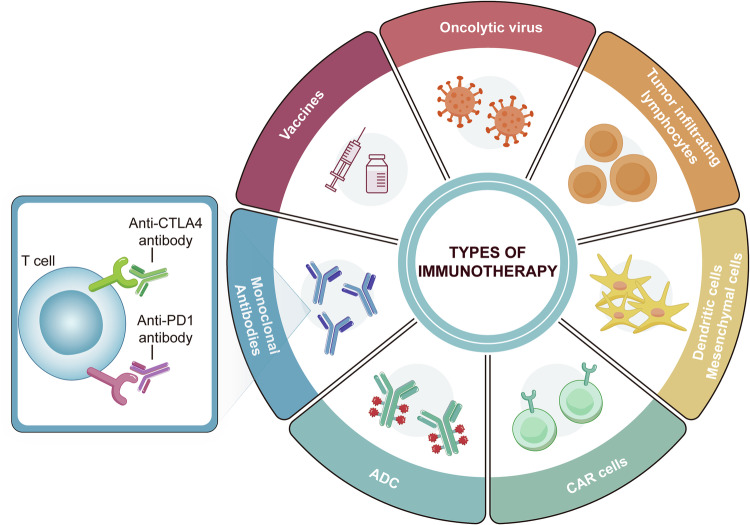
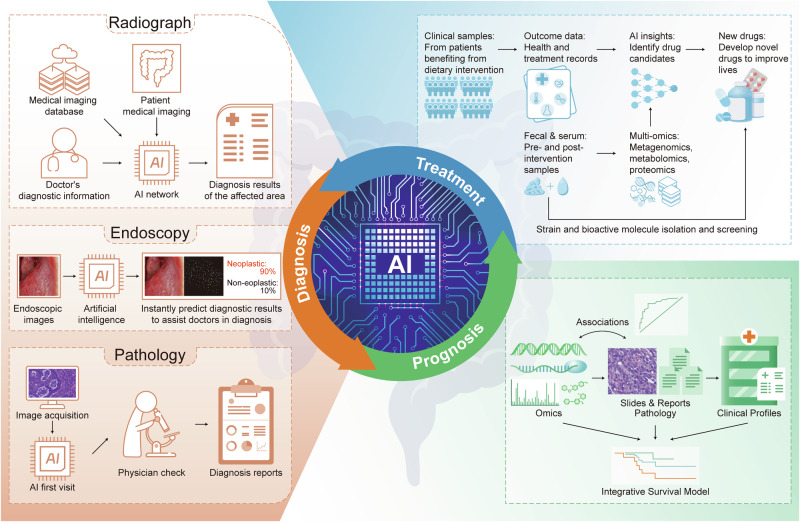
Colorectal cancer (CRC) remains one of the leading causes of cancer-related mortality worldwide. Its complexity is influenced by various signal transduction networks that govern cellular proliferation, survival, differentiation, and apoptosis. The pathogenesis of CRC is a testament to the dysregulation of these signaling cascades, which culminates in the malignant transformation of colonic epithelium. This review aims to dissect the foundational signaling mechanisms implicated in CRC, to elucidate the generalized principles underpinning neoplastic evolution and progression. We discuss the molecular hallmarks of CRC, including the genomic, epigenomic and microbial features of CRC to highlight the role of signal transduction in the orchestration of the tumorigenic process. Concurrently, we review the advent of targeted and immune therapies in CRC, assessing their impact on the current clinical landscape. The development of these therapies has been informed by a deepening understanding of oncogenic signaling, leading to the identification of key nodes within these networks that can be exploited pharmacologically. Furthermore, we explore the potential of integrating AI to enhance the precision of therapeutic targeting and patient stratification, emphasizing their role in personalized medicine. In summary, our review captures the dynamic interplay between aberrant signaling in CRC pathogenesis and the concerted efforts to counteract these changes through targeted therapeutic strategies, ultimately aiming to pave the way for improved prognosis and personalized treatment modalities in colorectal cancer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.74, 229–263 (2024). - PubMed
-
- ArnoldM, S. & Laversanne, M. Global patterns and trendsin colorecta lcancer incidence and mortality. Gut66, 683 (2017). - PubMed
-
- Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell144, 646–674 (2011). - PubMed
-
- Wood, L. D. et al. The genomic landscapes of human breast and colorectal cancers. Science318, 1108–1113 (2007). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
