

Replacement with sex steroids in hypopituitary men and women: implications for gender differences in morbidities and mortality
- PMID: 39370498
- PMCID: PMC11470859
- DOI: 10.1007/s11154-024-09897-7
Replacement with sex steroids in hypopituitary men and women: implications for gender differences in morbidities and mortality
Abstract
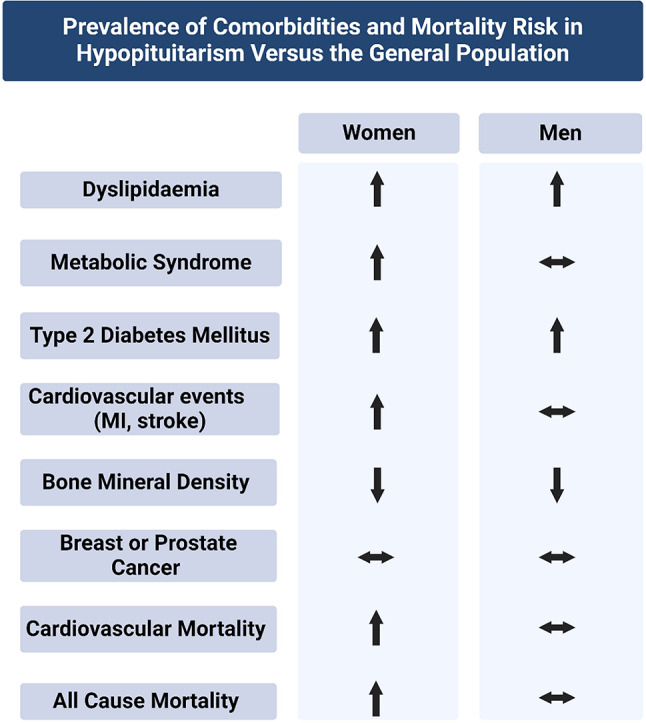
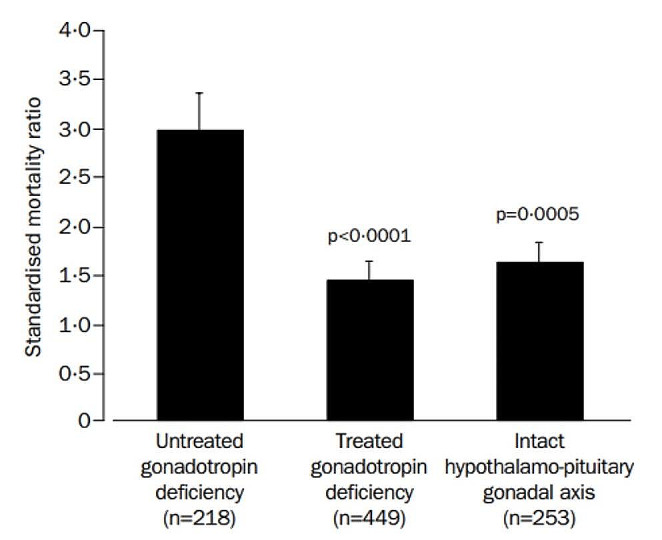
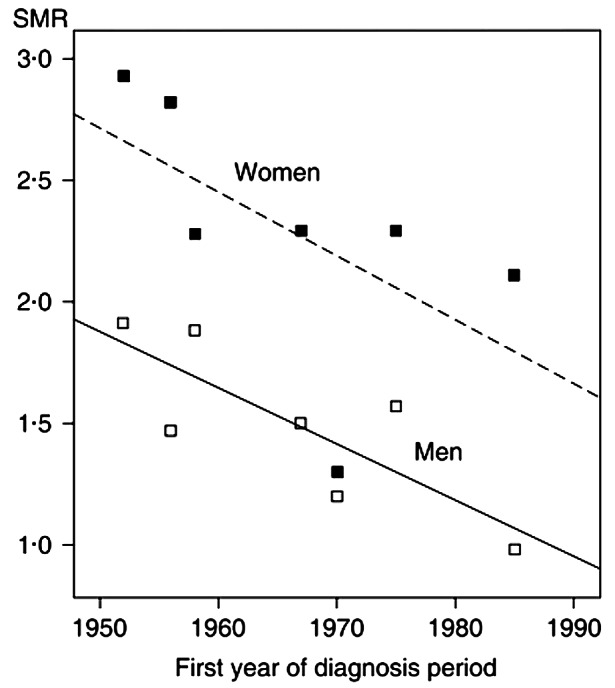
Hypopituitarism is a heterogenous disorder characterised by a deficiency in one or more anterior pituitary hormones. There are marked sex disparities in the morbidity and mortality experienced by patients with hypopituitarism. In women with hypopituitarism, the prevalence of many cardiovascular risk factors, myocardial infarction, stroke and mortality are significantly elevated compared to the general population, however in men, they approach that of the general population. The hypothalamic-pituitary-gonadal axis (HPG) is the most sexually dimorphic pituitary hormone axis. Gonadotropin deficiency is caused by a deficiency of either hypothalamic gonadotropin-releasing hormone (GnRH) or pituitary gonadotropins, namely follicle-stimulating hormone (FSH) and luteinising hormone (LH). HPG axis dysfunction results in oestrogen and testosterone deficiency in women and men, respectively. Replacement of deficient sex hormones is the mainstay of treatment in individuals not seeking fertility. Oestrogen and testosterone replacement in women and men, respectively, have numerous beneficial health impacts. These benefits include improved body composition, enhanced insulin sensitivity, improved atherogenic lipid profiles and increased bone mineral density. Oestrogen replacement in women also reduces the risk of developing type 2 diabetes mellitus. When women and men are considered together, untreated gonadotropin deficiency is independently associated with an increased mortality risk. However, treatment with sex hormone replacement reduces the mortality risk comparable to those with an intact gonadal axis. The reasons for the sex disparities in mortality remain poorly understood. Potential explanations include the reversal of women's natural survival advantage over men, premature loss of oestrogen's cardioprotective effect, less aggressive cardiovascular risk factor modification and inadequate oestrogen replacement in women with gonadotropin deficiency. Regrettably, historical inertia and unfounded concerns about the safety of oestrogen replacement in women of reproductive age have impeded the treatment of gonadotropin deficiency.
Keywords: Gonadotropin deficiency; Hypogonadotropic hypogonadism; Hypopituitarism; Mortality; Oestrogen; Sex hormone; Testosterone.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Hypopituitarism.Pituitary. 2006;9(4):335-42. doi: 10.1007/s11102-006-0416-5. Pituitary. 2006. PMID: 17077946 Review.
-
Effects of decreasing the frequency of gonadotropin-releasing hormone stimulation on gonadotropin secretion in gonadotropin-releasing hormone-deficient men and perifused rat pituitary cells.J Clin Invest. 1988 Jun;81(6):1725-33. doi: 10.1172/JCI113512. J Clin Invest. 1988. PMID: 3290251 Free PMC article.
-
Sex Steroid Levels in Women With Hypopituitarism: A Case-controlled Observational Study.J Clin Endocrinol Metab. 2024 Oct 15;109(11):2967-2978. doi: 10.1210/clinem/dgae197. J Clin Endocrinol Metab. 2024. PMID: 38570732 Free PMC article.
-
Correlation between integrated LH and FSH levels and the response to luteinizing hormone relasing factor (LRF).J Clin Endocrinol Metab. 1976 Dec;43(6):1240-9. doi: 10.1210/jcem-43-6-1240. J Clin Endocrinol Metab. 1976. PMID: 794076
-
Hormone replacement therapy in hypopituitarism.Expert Opin Pharmacother. 2004 May;5(5):1023-31. doi: 10.1517/14656566.5.5.1023. Expert Opin Pharmacother. 2004. PMID: 15155105 Review.
Cited by
-
Association of cardiovascular-kidney-metabolic index with all-cause mortality during hospitalization in critically ill patients: a retrospective cohort study from MIMIC IV2.2.Front Cardiovasc Med. 2024 Dec 9;11:1513212. doi: 10.3389/fcvm.2024.1513212. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39717440 Free PMC article.
References
-
- Higham CE, Johannsson G, Shalet SM, Hypopituitarism. Lancet. 2016;388(10058):2403–15. 10.1016/S0140-6736(16)30053-8. - PubMed
-
- Regal M, Páramo C, Sierra SM, Garcia-Mayor RV. Prevalence and incidence of hypopituitarism in an adult caucasian population in northwestern Spain. Clin Endocrinol (Oxf). 2001;55(6):735–40. 10.1046/j.1365-2265.2001.01406.x. - PubMed
-
- Rosén T, Bengtsson BA. Premature mortality due to cardiovascular disease in hypopituitarism. Lancet. 1990;336(8710):285–8. 10.1016/0140-6736(90)91812-o. - PubMed
-
- Tomlinson JW, Holden N, Hills RK, Wheatley K, Clayton RN, Bates AS, et al. Association between premature mortality and hypopituitarism. West Midlands prospective Hypopituitary Study Group. Lancet. 2001;357(9254):425–31. 10.1016/s0140-6736(00)04006-x. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
