

This is a preprint.
Pediatric Long COVID Subphenotypes: An EHR-based study from the RECOVER program
- PMID: 39371163
- PMCID: PMC11451761
- DOI: 10.1101/2024.09.17.24313742
Pediatric Long COVID Subphenotypes: An EHR-based study from the RECOVER program
Update in
-
Pediatric Long COVID Subphenotypes: An EHR-based study from the RECOVER program.PLOS Digit Health. 2025 Apr 10;4(4):e0000747. doi: 10.1371/journal.pdig.0000747. eCollection 2025 Apr. PLOS Digit Health. 2025. PMID: 40208885 Free PMC article.
Abstract
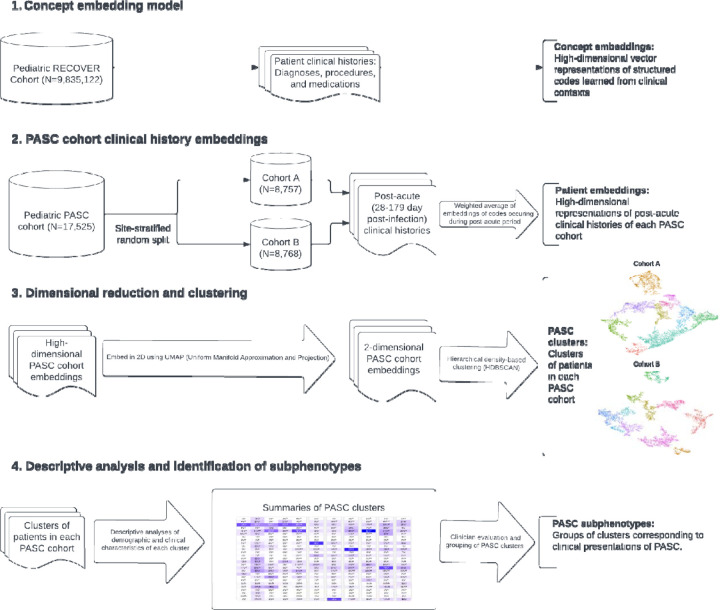
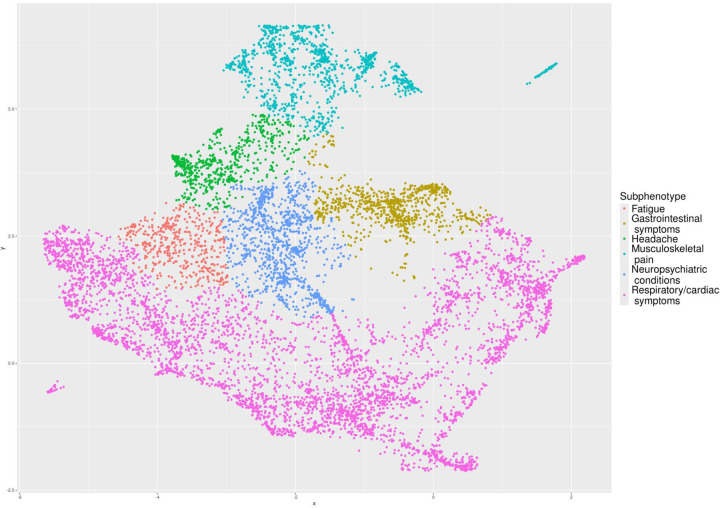
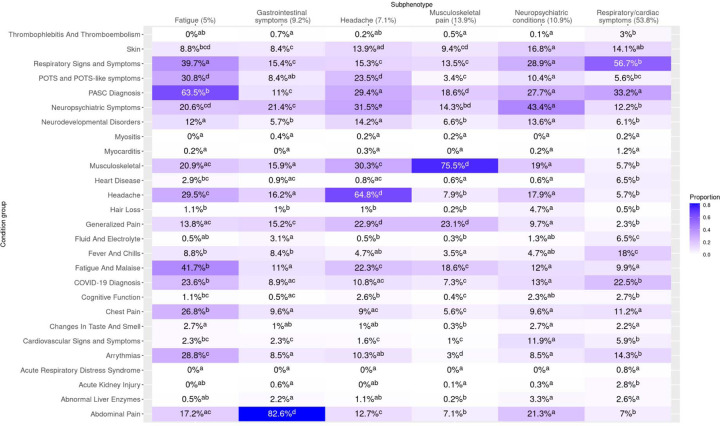
Pediatric Long COVID has been associated with a wide variety of symptoms, conditions, and organ systems, but distinct clinical presentations, or subphenotypes, are still being elucidated. In this exploratory analysis, we identified a cohort of pediatric (age <21) patients with evidence of Long COVID and no pre-existing complex chronic conditions using electronic health record data from 38 institutions and used an unsupervised machine learning-based approach to identify subphenotypes. Our method, an extension of the Phe2Vec algorithm, uses tens of thousands of clinical concepts from multiple domains to represent patients' clinical histories to then identify groups of patients with similar presentations. The results indicate that cardiorespiratory presentations are most common (present in 54% of patients) followed by subphenotypes marked (in decreasing order of frequency) by musculoskeletal pain, neuropsychiatric conditions, gastrointestinal symptoms, headache, and fatigue.
Conflict of interest statement
Dr. Jhaveri is a consultant for AstraZeneca, Seqirus, Dynavax, receives an editorial stipend from Elsevier and Pediatric Infectious Diseases Society and royalties from Up To Date/Wolters Kluwer. Dr. Rao reports prior grant support from GSK and Biofire and is a consultant for Sequiris. Dr Bailey has received grants from Patient-Centered Outcomes Research Institute. Dr. Brill received support from Novartis and Regeneron Pharmaceuticals within the last year. Dr. Horne is a member of the advisory boards of Opsis Health and Lab Me Analytics, a consultant to Pfizer regarding risk scores (funds paid to Intermountain), and an inventor of risk scores licensed by Intermountain to Alluceo and CareCentra and is site PI of a COVID-19 grant from the Task Force for Global Health, site PI of grants from the Patient-Centered Outcomes Research Institute, a member of the advisory board of Opsis Health, and previously consulted for Pfizer regarding risk scores (funds paid to Intermountain). All other authors have no conflicts of interest to disclose.
Figures
References
-
- Rao S, Lee GM, Razzaghi H, Lorman V, Mejias A, Pajor NM, et al. Clinical features and burden of post-acute sequelae of SARS-CoV-2 infection in children and adolescents: an exploratory EHR-based cohort study from the RECOVER program. MedRxiv Prepr Serv Health Sci 2022:2022.05.24.22275544. 10.1101/2022.05.24.22275544. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources