

Empowering adolescents living with perinatally-acquired HIV: tailored CD4+ count assessment for optimized care, the EDCTP READY-study
- PMID: 39371336
- PMCID: PMC11450861
- DOI: 10.3389/fmed.2024.1457501
Empowering adolescents living with perinatally-acquired HIV: tailored CD4+ count assessment for optimized care, the EDCTP READY-study
Abstract
Background: The elevated rate of AIDS-related mortality in Sub-Saharan Africa among adolescents living with HIV (ALHIV) is influenced by various factors, notably immunosuppression, within a framework of limited therapeutic alternatives. We aimed to enhance the management of pediatric HIV by assessing the immune response and associated factors in perinatally-infected ALHIV on antiretroviral therapy (ART) in Cameroon.
Methods: A cohort study was conducted from 2018-2020 among 271 ART-experienced ALHIV in Cameroon. Sociodemographic data, immunological (CD4), and virological (plasma viral load, PVL) responses were measured at enrolment (T0), 6-months (T1), and 12-months (T2) using PIMA CD4 (Abbott/Pantech (Pty) Ltd) and Abbott Applied Biosystem platform (Real-Time PCR m2000RT) respectively. Immunological failure (IF) was defined as absolute CD4 < 250 cells/mm3, and Virological failure (VF) as PVL ≥ 1,000 copies/ml. A linear mixed-effects model with R version 4.4.1 was used to estimate both fixed and random effects, with significance set at p < 0.05.
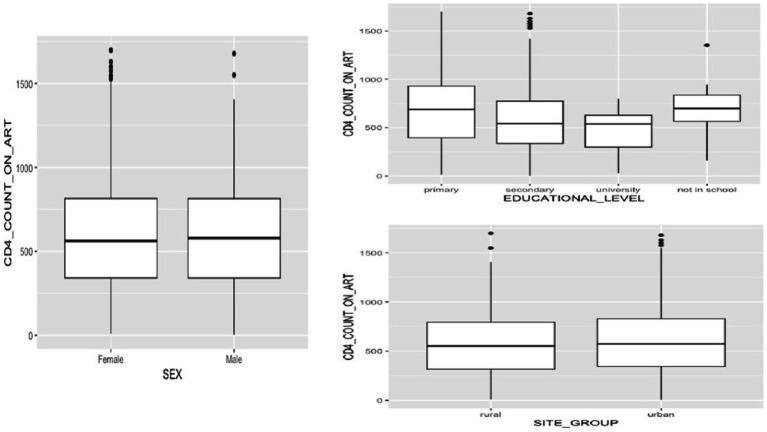
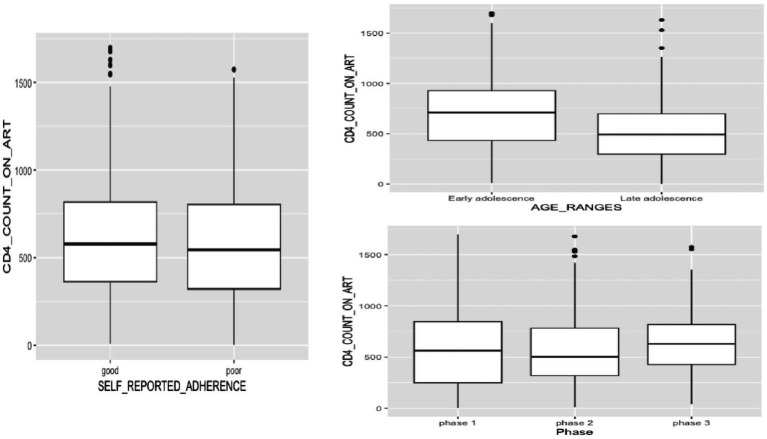
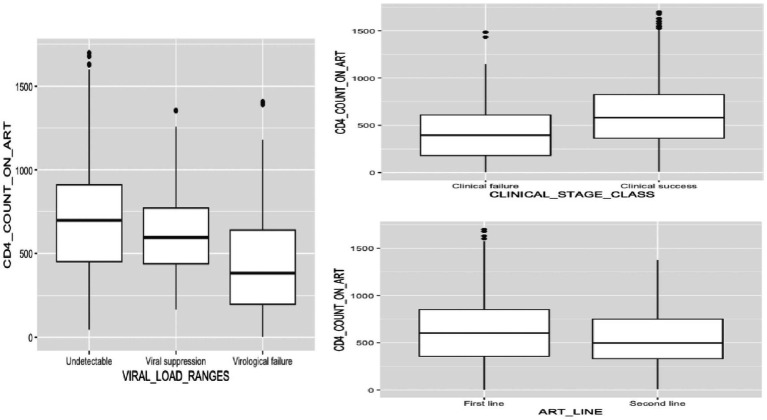
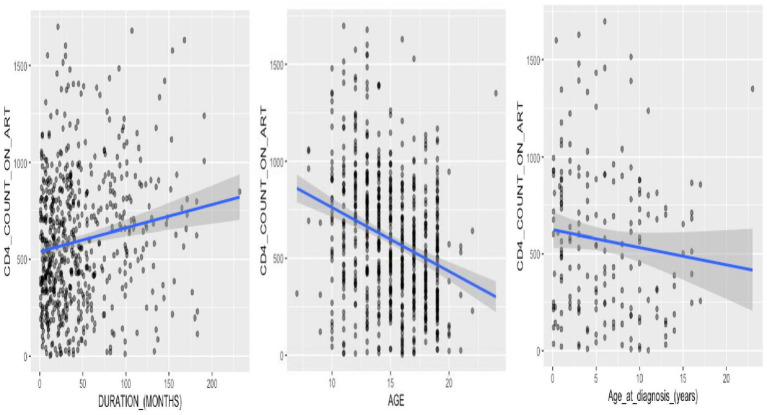
Results: Of the 271 perinatally-infected ALHIV enrolled over three phases, females were predominant (55.7, 55.1, and 56.0%); median age was 14 (IQR: 12-17); majority of the participants were followed-up in urban areas (77.5, 74.5, and 78.6%); and the age distribution favored older adolescents (48.7, 61.2, and 58.5%). Most participants achieved clinical success (93.1, 89.7, 88.9%), predominantly on first-line ART (80.8, 66.2, and 53.0%), with good adherence (64.2, 58.9, and 64.5%). Most participants had secondary education (67.2, 70.1, and 67.5%). Median CD4+ counts fluctuated overtime, with values of 563 (IQR: 249.0-845.0), 502 (IQR: 319.0-783.5), and 628 (IQR: 427.5-817.5), respectively. Of note, being male was linked to a reduction in CD4+ count compared to females, [-200.63 (-379.32 to -21.95), p = 0.028]. Similarly, late adolescence was associated with lower CD4+ counts compared to early adolescence, [-181.08 (-301.08 to -61.09), p = 0.003]. Moreover, participants experiencing VF showed significantly lower CD4+ counts compared to those with undetectable viral loads, [-353.08 (-465.81 to -240.36), p < 0.001]. Additionally, there was a marginally significant interaction between male gender and secondary educational level, [209.78 (-6.94-426.51), p = 0.058].
Conclusion: Among perinatally-infected ALHIV, age, gender, educational level, and virological status are key factors influencing their immune health and treatment outcomes. Prioritizing targeted interventions and close monitoring within these subgroups is crucial for optimal management, employing holistic care strategies that consider not only medical interventions but also psychosocial support and education.
Keywords: CD4 cell count; Cameroon; HIV; adolescents; immune monitoring.
Copyright © 2024 Togna Pabo, Kengni Ngueko, Nka, Santoro, Bouba, Chenwi, Ngoufack Jagni Semengue, Takou, Teto, Dambaya, Nyasa, Tommo Tchouaket, Beloumou, Djupsa Ndjeyep, Ka’e, Tekoh, Ayuk Ngwese, Etame, Mundo, Kamgaing, Sosso, Ndip, Colizzi, Cecchereni-Silberstein, Ndjolo and Fokam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- UNAIDS . (n.d.) Statistiques mondiales sur le VIH. Available online at: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_... (Accessed September 23, 2020)
-
- Global AIDS Update . (2016). XXX.
-
- Bekker L-G, Hosek S. HIV and adolescents: focus on young key populations. J Int AIDS Soc. 18:20076. doi: 10.7448/IAS.18.2.20076 - DOI
-
- Fish R, Judd A, Jungmann E, O'Leary C, Foster C, HIV Young Persons Network (HYPNet) . Mortality in perinatally HIV-infected young people in England following transition to adult care: an HIV young persons network (HYPNet) audit. HIV Med. (2014) 15:239–44. doi: 10.1111/hiv.12091, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous