

Effect of automated identification of antimicrobial stewardship opportunities for suspected urinary tract infections
- PMID: 39371441
- PMCID: PMC11450662
- DOI: 10.1017/ash.2024.437
Effect of automated identification of antimicrobial stewardship opportunities for suspected urinary tract infections
Abstract
Objective: We aimed to determine whether automated identification of antibiotic targeting suspected urinary tract infection (UTI) shortened the time to antimicrobial stewardship (AS) intervention.
Design: Retrospective before-and-after study.
Setting: Tertiary and quaternary care academic medical center.
Patients: Emergency department (ED) or admitted adult patients meeting best practice alert (BPA) criteria during pre- and post-BPA periods.
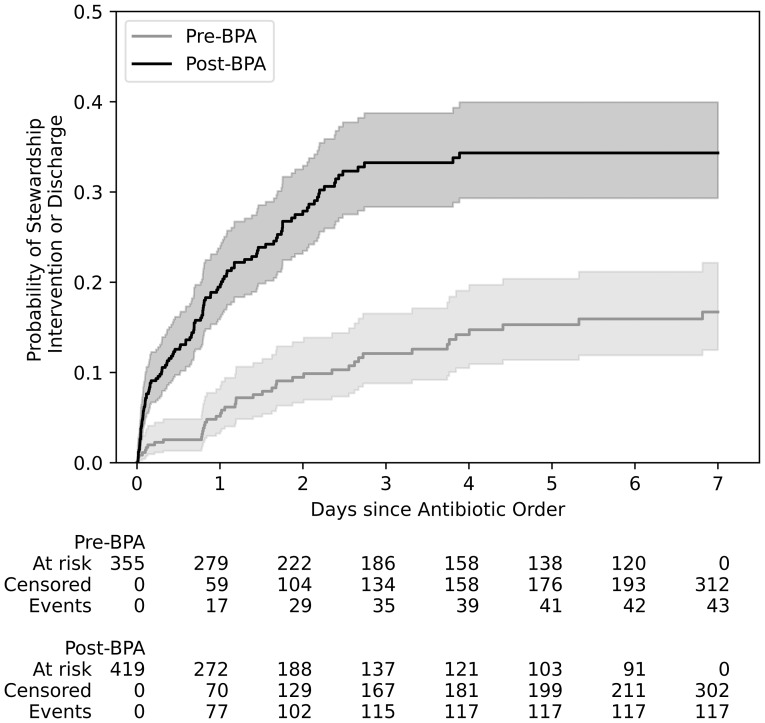
Methods: We developed a BPA to alert AS pharmacists of potential ASB triggered by the following criteria: ED or admitted status, antibiotic order with genitourinary indication, and a preceding urinalysis with ≤ 10 WBC/hpf. We evaluated the median time from antibiotic order to AS intervention and overall percent of UTI-related interventions among patients in pre-BPA (01/2020-12/2020) and post-BPA (04/15/2021-04/30/2022) periods.
Results: 774 antibiotic orders met inclusion criteria: 355 in the pre- and 419 in the post-BPA group. 43 (35 UTI-related) pre-BPA and 117 (94 UTI-related) post-BPA interventions were documented. The median time to intervention was 28 hours (IQR 18-65) in the pre-BPA group compared to 16 hours (IQR 2-34) in the post-BPA group (P < 0.01). Despite absent pyuria, there were six cases with gram-negative bacteremia presumably from a urinary source.
Conclusions: Automated identification of antibiotics targeting UTI without pyuria on urinalysis reduced the time to stewardship intervention and increased the rate of UTI-specific interventions. Clinical decision support aided in the efficiency of AS review and syndrome-targeted impact, but cases still required AS clinical review.
© The Author(s) 2024.
Conflict of interest statement
S.D.A. reports support from the Centers from Disease Control and Prevention (grant nos. 5U54CK000616-02 and SHEPheRD 75D30121D12733-D5-E003), National Institutes of Health (National Institute of Diabetes and Digestive and Kidney Diseases grant no. K12DK100024), the Society for Healthcare Epidemiology of America, and as well as prior consulting fees from Locus Biosciences, Sysmex America, GlaxoSmithKline, bioMérieux, and the Infectious Diseases Society of America. Additionally, S.D.A is an employee of GSK/ViiV Health care as of July 1, 2024 and holds stock in GlaxoSmithKline.
Figures


References
-
- Doernberg SB, Abbo LM, Burdette SD, et al. Essential resources and strategies for antibiotic stewardship programs in the acute care setting. Clin Infect Dis 2018;67:1168–1174. - PubMed
-
- Warren JW, Tenney JH, Hoopes JM, Muncie HL, Anthony WC. A prospective microbiologic study of bacteriuria in patients with chronic indwelling urethral catheters. J Infect Dis 1982;146:719–23. - PubMed
-
- Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the infectious diseases society of America. Clin Infect Dis 2019;68:e83–75. - PubMed
-
- Nicolle LE, Mayhew WJ, Bryan L. Prospective randomized comparison of therapy and no therapy for asymptomatic bacteriuria in institutionalized elderly women. Am J Med 1987;83:27–33. - PubMed
-
- Harding GKM, Zhanel GG, Nicolle LE, Cheang M; manitoba diabetes urinary tract infection study group. Antimicrobial treatment in diabetic women with asymptomatic bacteriuria. N Eng J Med 2002;347:1576–83. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous