

Estimating the impact of physician risky-prescribing on the network structure underlying physician shared-patient relationships
- PMID: 39372037
- PMCID: PMC11450072
- DOI: 10.1007/s41109-024-00670-y
Estimating the impact of physician risky-prescribing on the network structure underlying physician shared-patient relationships
Abstract
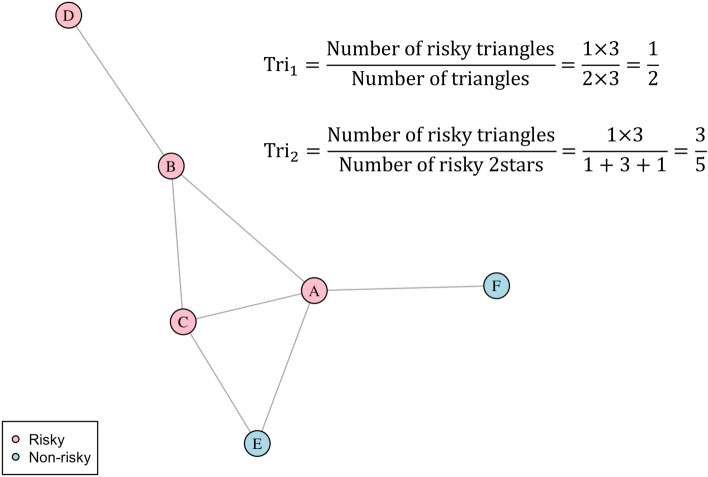
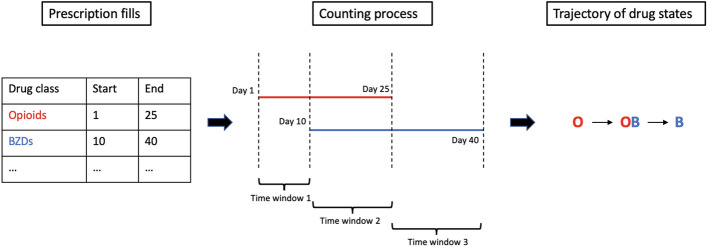
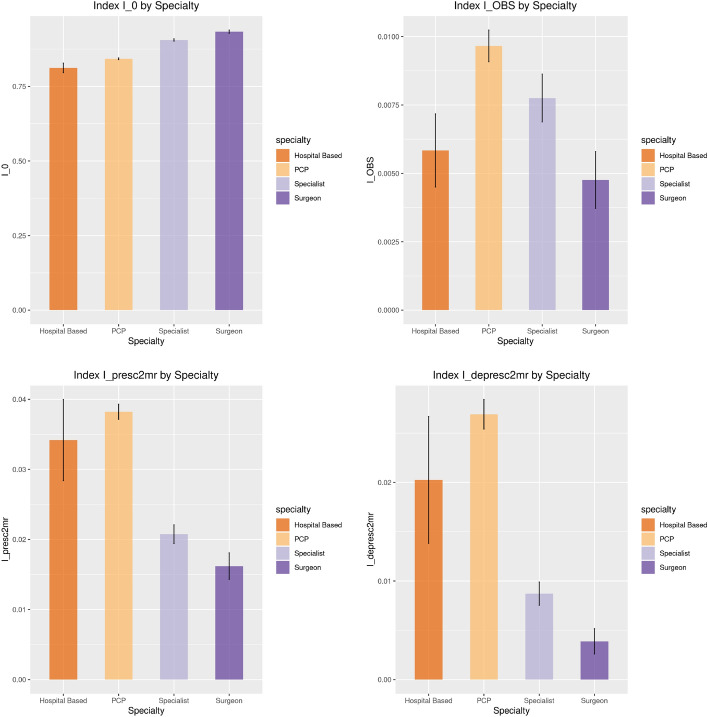
Social network analysis and shared-patient physician networks have become effective ways of studying physician collaborations. Assortative mixing or "homophily" is the network phenomenon whereby the propensity for similar individuals to form ties is greater than for dissimilar individuals. Motivated by the public health concern of risky-prescribing among older patients in the United States, we develop network models and tests involving novel network measures to study whether there is evidence of homophily in prescribing and deprescribing in the specific shared-patient network of physicians linked to the US state of Ohio in 2014. Evidence of homophily in risky-prescribing would imply that prescribing behaviors help shape physician networks and would suggest strategies for interventions seeking to reduce risky-prescribing (e.g., strategies to directly reduce risky prescribing might be most effective if applied as group interventions to risky prescribing physicians connected through the network and the connections between these physicians could be targeted by tie dissolution interventions as an indirect way of reducing risky prescribing). Furthermore, if such effects varied depending on the structural features of a physician's position in the network (e.g., by whether or not they are involved in cliques-groups of actors that are fully connected to each other-such as closed triangles in the case of three actors), this would further strengthen the case for targeting groups of physicians involved in risky prescribing and the network connections between them for interventions. Using accompanying Medicare Part D data, we converted patient longitudinal prescription receipts into novel measures of the intensity of each physician's risky-prescribing. Exponential random graph models were used to simultaneously estimate the importance of homophily in prescribing and deprescribing in the network beyond the characteristics of physician specialty (or other metadata) and network-derived features. In addition, novel network measures were introduced to allow homophily to be characterized in relation to specific triadic (three-actor) structural configurations in the network with associated non-parametric randomization tests to evaluate their statistical significance in the network against the null hypothesis of no such phenomena. We found physician homophily in prescribing and deprescribing. We also found that physicians exhibited within-triad homophily in risky-prescribing, with the prevalence of homophilic triads significantly higher than expected by chance absent homophily. These results may explain why communities of prescribers emerge and evolve, helping to justify group-level prescriber interventions. The methodology may be applied, adapted or generalized to study homophily and its generalizations on other network and attribute combinations involving analogous shared-patient networks and more generally using other kinds of network data underlying other kinds of social phenomena.
Keywords: Deprescribing; Homophily; Quantifying polypharmacy; Risky prescribing; Shared-patient physician network; State-space; Transition matrix.
© The Author(s) 2024.
Conflict of interest statement
Competing interestsThe authors declare no potential Conflict of interest.
Figures

Update of
-
Estimating the impact of physician risky-prescribing on the network structure underlying physician shared-patient relationships.Res Sq [Preprint]. 2024 Mar 26:rs.3.rs-4139630. doi: 10.21203/rs.3.rs-4139630/v1. Res Sq. 2024. Update in: Appl Netw Sci. 2024;9(1):63. doi: 10.1007/s41109-024-00670-y. PMID: 38585838 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous