

Should Hypertonic Saline Be Considered for the Treatment of Intracranial Hypertension? A Review of Current Evidence and Clinical Practices
- PMID: 39372110
- PMCID: PMC11450342
- DOI: 10.13004/kjnt.2024.20.e35
Should Hypertonic Saline Be Considered for the Treatment of Intracranial Hypertension? A Review of Current Evidence and Clinical Practices
Abstract
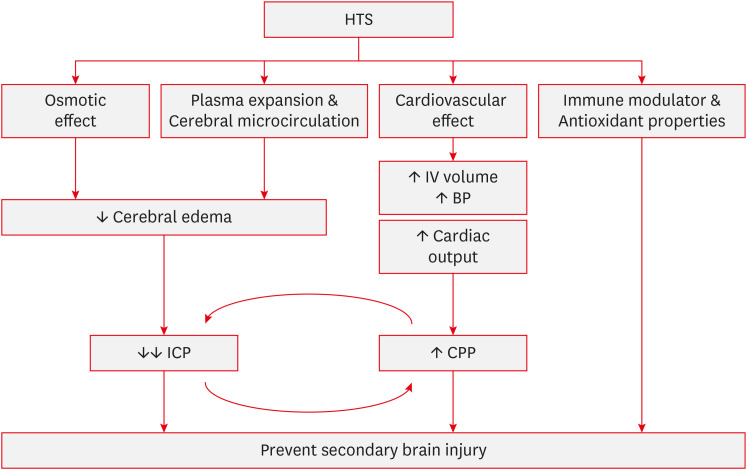
Intracranial hypertension (IH) is a critical neurological emergency that requires prompt intervention because failure to treat it properly can lead to severe outcomes, including secondary brain injury. Traditionally, mannitol (MNT) has been the cornerstone of hyperosmolar therapy. However, the use of hypertonic saline (HTS) has become increasingly important because of its unique advantages. Both HTS and MNT effectively reduce intracranial pressure by creating an osmotic gradient that draws fluid from brain tissue. However, unlike MNT, HTS does not induce diuresis or significantly lower blood pressure, making it more favorable for maintaining cerebral perfusion. Additionally, HTS does not cause rebound edema and carries a lower risk of renal injury than MNT. However, it is important to note that the use of HTS comes with potential risks, such as hypernatremia, hyperchloremia, and fluid overload. Due to its unique properties, HTS is a crucial agent in the management of IH, and understanding its appropriate use is essential to optimize patient outcomes.
Keywords: Brain edema; Intracranial hypertension/drug therapy; Mannitol; Saline solution, hypertonic.
Copyright © 2024 Korean Neurotraumatology Society.
Conflict of interest statement
Conflict of Interest: The authors have no financial conflicts of interest.
Figures
Similar articles
-
Hyperosmolar therapy in the treatment of severe head injury in children: mannitol and hypertonic saline.AACN Clin Issues. 2005 Apr-Jun;16(2):199-211. doi: 10.1097/00044067-200504000-00011. AACN Clin Issues. 2005. PMID: 15876888 Review.
-
Hypertonic saline versus other intracranial pressure-lowering agents for people with acute traumatic brain injury.Cochrane Database Syst Rev. 2019 Dec 30;12(12):CD010904. doi: 10.1002/14651858.CD010904.pub2. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2020 Jan 17;1:CD010904. doi: 10.1002/14651858.CD010904.pub3. PMID: 31886900 Free PMC article. Updated.
-
Hypertonic saline for the management of raised intracranial pressure after severe traumatic brain injury.Ann N Y Acad Sci. 2015 May;1345:83-8. doi: 10.1111/nyas.12704. Epub 2015 Feb 27. Ann N Y Acad Sci. 2015. PMID: 25726965
-
Hypertonic saline versus other intracranial pressure-lowering agents for people with acute traumatic brain injury.Cochrane Database Syst Rev. 2020 Jan 17;1(1):CD010904. doi: 10.1002/14651858.CD010904.pub3. Cochrane Database Syst Rev. 2020. PMID: 31978260 Free PMC article.
-
Hypertonic saline reduces cumulative and daily intracranial pressure burdens after severe traumatic brain injury.J Neurosurg. 2015 Jan;122(1):202-10. doi: 10.3171/2014.10.JNS132545. J Neurosurg. 2015. PMID: 25380107 Clinical Trial.
References
-
- Bourdeaux CP, Brown JM. Randomized controlled trial comparing the effect of 8.4% sodium bicarbonate and 5% sodium chloride on raised intracranial pressure after traumatic brain injury. Neurocrit Care. 2011;15:42–45. - PubMed
-
- Bulger EM, Hoyt DB. Hypertonic resuscitation after severe injury: is it of benefit? Adv Surg. 2012;46:73–85. - PubMed
-
- Burke AM, Quest DO, Chien S, Cerri C. The effects of mannitol on blood viscosity. J Neurosurg. 1981;55:550–553. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
