

Carbohydrate Restriction-Induced Elevations in LDL-Cholesterol and Atherosclerosis: The KETO Trial
- PMID: 39372369
- PMCID: PMC11450898
- DOI: 10.1016/j.jacadv.2024.101109
Carbohydrate Restriction-Induced Elevations in LDL-Cholesterol and Atherosclerosis: The KETO Trial
Abstract
Background: Increases in low-density lipoprotein cholesterol (LDL-C) can occur on carbohydrate restricted ketogenic diets. Lean metabolically healthy individuals with a low triglyceride-to-high-density lipoprotein cholesterol ratio appear particularly susceptible, giving rise to the novel "lean mass hyper-responder" (LMHR) phenotype.
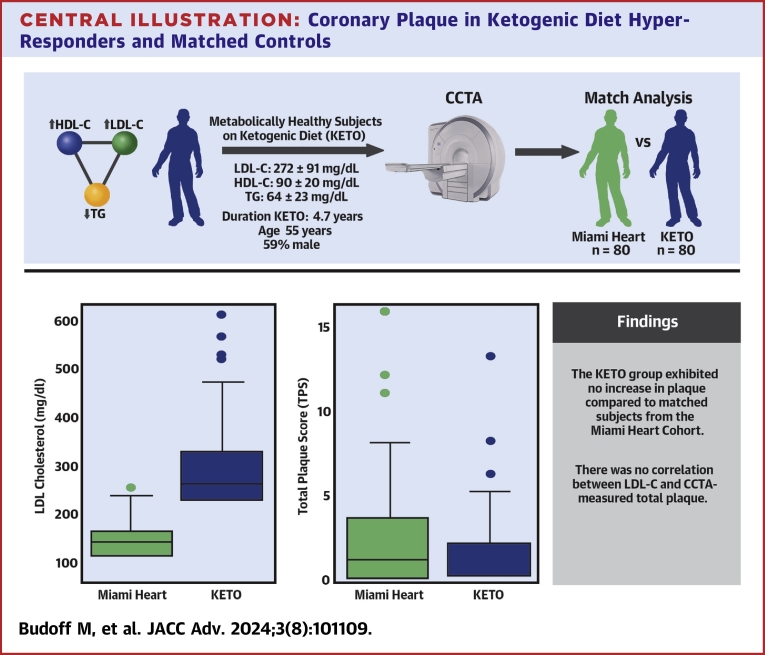
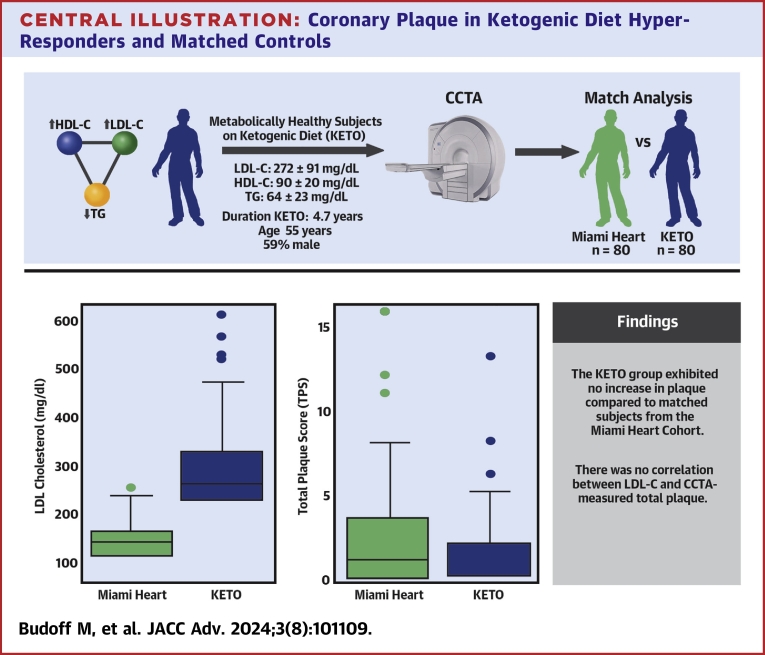
Objectives: The purpose of the study was to assess coronary plaque burden in LMHR and near-LMHR individuals with LDL-C ≥190 mg/dL (ketogenic diet [KETO]) compared to matched controls with lower LDL-C from the Miami Heart (MiHeart) cohort.
Methods: There were 80 KETO individuals with carbohydrate restriction-induced LDL-C ≥190 mg/dL, high-density lipoprotein cholesterol ≥60 mg/dL, and triglyceride levels ≤80 mg/dL, without familial hypercholesterolemia, matched 1:1 with MiHeart subjects for age, gender, race, hyperlipidemia, hypertension, and smoking status. Coronary artery calcium and coronary computed tomography angiography (CCTA) were used to compare coronary plaque between groups and correlate LDL-C to plaque levels.
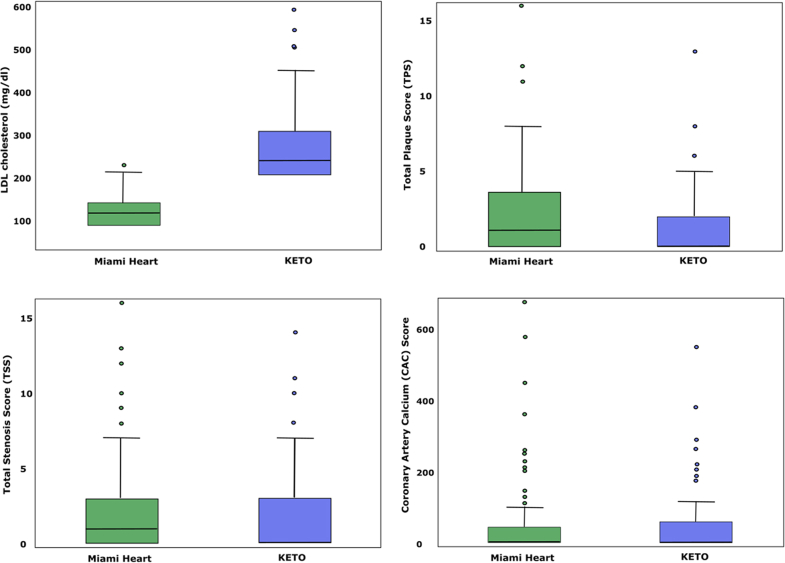
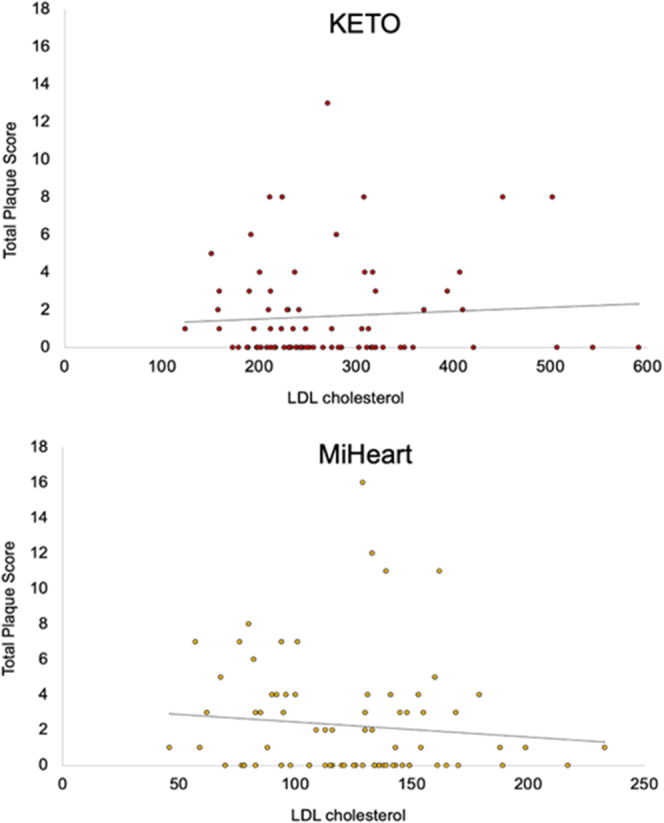
Results: The matched mean age was 55.5 years, with a mean LDL-C of 272 (maximum LDL-C of 591) mg/dl and a mean 4.7-year duration on a KETO. There was no significant difference in coronary plaque burden in the KETO group as compared to MiHeart controls (mean LDL 123 mg/dL): coronary artery calcium score (median 0 [IQR: 0-56]) vs (1 [IQR: 0-49]) (P = 0.520) CCTA total plaque score (0 [IQR: 0-2] vs [IQR: 0-4]) (P = 0.357). There was also no correlation between LDL-C level and CCTA coronary plaque.
Conclusions: Coronary plaque in metabolically healthy individuals with carbohydrate restriction-induced LDL-C ≥190 mg/dL on KETO for a mean of 4.7 years is not greater than a matched cohort with 149 mg/dL lower average LDL-C. There is no association between LDL-C and plaque burden in either cohort. (Diet-induced Elevations in LDL-C and Progression of Atherosclerosis [Keto-CTA]; NCT057333255).
Keywords: LDL cholesterol; atherosclerosis; coronary CT angiography; ketogenic diet; lean mass hyper-responder; plaque.
© 2024 The Authors.
Conflict of interest statement
This study was funded by the Citizen Science Foundation, 7320 S Rainbow Blvd, #102-182, Las Vegas, NV, United States. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524–533. - PubMed
-
- Kohli-Lynch C.N., Thanassoulis G., Moran A.E., Sniderman A.D. The clinical utility of apoB versus LDL-C/non-HDL-C. Clin Chim Acta. 2020;508:103–108. - PubMed
-
- Wang N., Woodward M., Huffman M.D., Rodgers A. Compounding Benefits of cholesterol-lowering therapy for the reduction of major cardiovascular events: Systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2022;15(6) - PubMed
