

Bone turnover, areal BMD, and bone microarchitecture by second-generation high-resolution peripheral quantitative computed tomography in transfusion-dependent thalassemia
- PMID: 39372604
- PMCID: PMC11450324
- DOI: 10.1093/jbmrpl/ziae117
Bone turnover, areal BMD, and bone microarchitecture by second-generation high-resolution peripheral quantitative computed tomography in transfusion-dependent thalassemia
Abstract
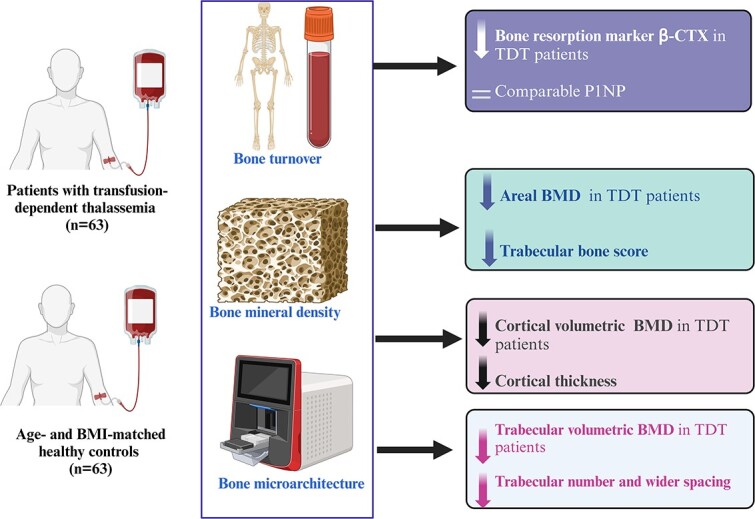
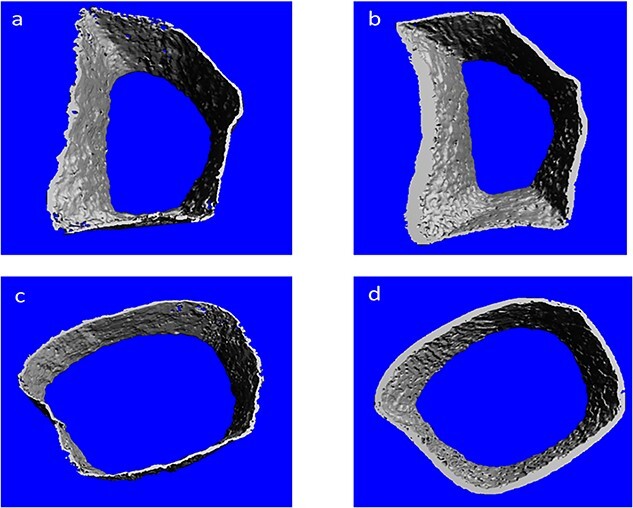
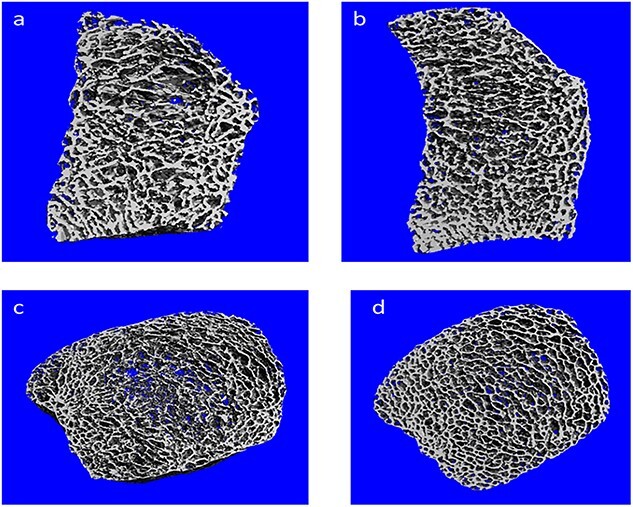
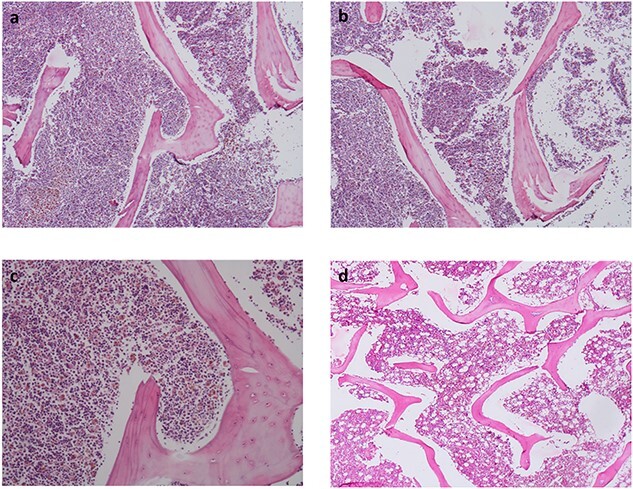
Thalassemic osteopathy includes low bone mass and impaired bone microarchitecture. We aimed to evaluate the prevalence and determinants of bone quantity (osteoporosis) and quality (microarchitecture) in a cohort of adult patients with transfusion-dependent thalassemia (TDT). Patients with TDT (n = 63) and age- and BMI-matched controls (n = 63) were recruited in the study. Areal bone mineral density (BMD) was measured using DXA Hologic scanner. P1NP and β-CTX were estimated by electrochemiluminescence assay. Bone geometry and volumetric BMD (vBMD) were estimated by second-generation high-resolution peripheral quantitative computed tomography. Bone turnover marker β-CTX was significantly lower in the TDT group, but there was no difference in P1NP levels. Low bone mass (Z ≤ -2) was present in greater proportion of patients both at lumbar spine (LS) (54 vs 0%; p = .001) and femoral neck (FN) (33 vs 8%; p = .001). Hypogonadism was associated with low BMD at FN (OR 10.0; 95% CI, 1.2-86; p = .01) and low hemoglobin with low BMD at LS (OR 1.58; 95% CI, 0.96-2.60; p = .07). The mean trabecular bone score was also significantly lower in patients compared with controls (1.261 ± 0.072 vs 1.389 ± 0.058). Total, cortical and trabecular vBMD were significantly lower in cases than controls. The trabecular number and cortical thickness were significantly lower and trabecular separation higher in cases than controls. Adults with TDT have significantly lower areal, cortical and trabecular vBMD. The bone microarchitecture is also significantly impaired in terms of lower number and wider spacing of trabeculae as well as lower cortical thickness and area at both radius and tibia.
Keywords: HR-pQCT; bone microarchitecture; ferritin; iron overload; osteoporosis; thalassemia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
