

Spinal cord infarction: A systematic review and meta-analysis of patient's characteristics, diagnosis accuracy, management, and outcome
- PMID: 39372971
- PMCID: PMC11450783
- DOI: 10.25259/SNI_477_2024
Spinal cord infarction: A systematic review and meta-analysis of patient's characteristics, diagnosis accuracy, management, and outcome
Abstract
Background: Acute spinal cord infarction (SCI) is a rare ischemic vascular lesion. It is difficult to diagnose during the acute phase because the clinical features can vary widely, and the diffusion-weighted imaging of spinal cord magnetic resonance imaging (MRI) often fails to detect any obvious abnormality. The first aim of this study was to describe the SCI patients' characteristics, evaluate the accuracy of its diagnosis tools and management, and then find the strength of the effect of spinal surgical decompression on the patient's outcome.
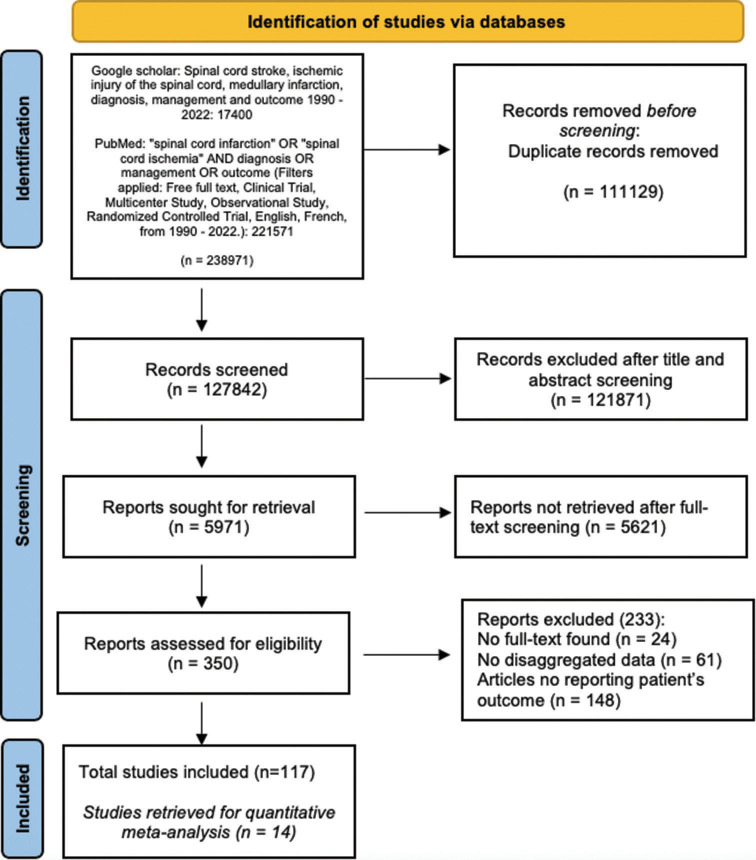
Methods: A PubMed keyword and Boolean search using ("spinal cord infarction" OR "spinal cord ischemia" AND diagnosis OR management OR outcome) returned 221,571 results by applying filters. We added 17,400 results from Google Scholar. Fourteen studies were included in the quantitative meta-analysis of mean differences.
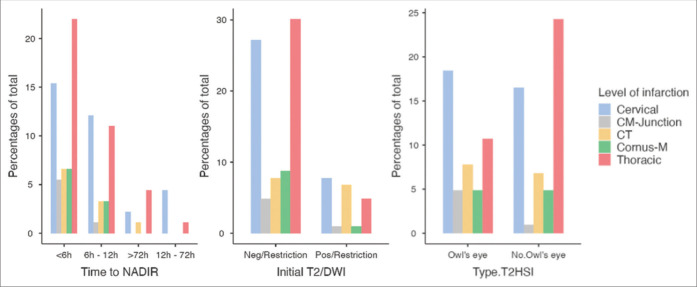
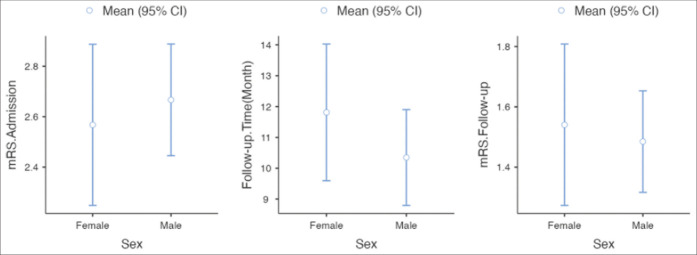
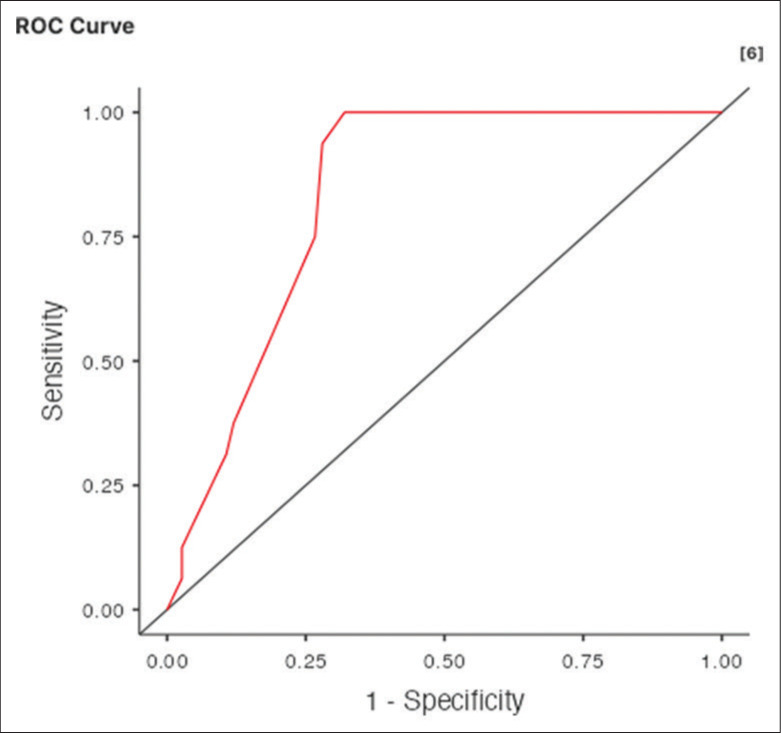
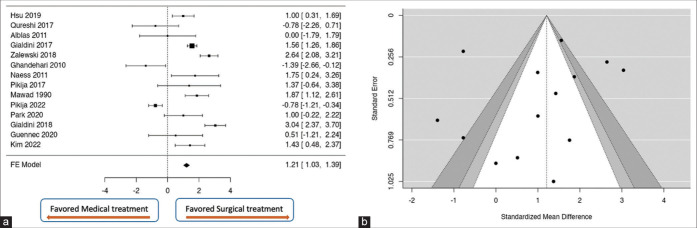
Results: The Time to Nadir was <6 h (56.1%), 6-12 h (30.7%), 12-72 h (5.4%), and more than 72 h (7.8%). The higher proportion of Owl's eye findings in the MRI was reported at the cervical level (39.6%) and thoracic level (22.9%) P = 0.031. The T2DWI has a moderate accuracy (area under the curve = 0.835) in detecting the T2 hypersignal intensity (T2HSI) at the hyperacute time to NADIR (<6 h). The median modified Rankin Scale (mRS) at admission was 3 (2-3), and after a follow-up duration of 12 months (6-15.5), the median mRS was reported to be 1 (1-2). About 68.9% benefited from medical treatment and physiotherapy, whereas spinal surgical decompression was done in 22.8%. Seventy percent of the overall studies favor spinal surgical decompression, with the estimated average standardized mean difference between medical and surgical treatment being = 1.2083 (95% confidence interval: 1.0250-1.3917).
Conclusion: The T2DWI has moderate accuracy in detecting the T2HSI at the hyperacute time (NADIR <6 h). Even though surgical decompression favored good outcomes, medical treatment with physiotherapy was mostly used for the management of SCI.
Keywords: Diagnosis; Management and outcome; Patient characteristics; Spinal cord infarction; Spinal cord ischemia.
Copyright: © 2024 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Alcanyis-Alberola M, Giner-Pascual M, Salinas-Huertas S, Gutiérrez-Delgado M. Iatrogenic spinal cord injury: An observational study. Spinal Cord. 2011;49:1188–92. - PubMed
-
- Badhiwala JH, Ahuja CS, Fehlings MG. Time is spine: A review of translational advances in spinal cord injury. J Neurosurg. 2018;30:1–18. - PubMed
-
- Bankole ND, Janot K, Listrat A, Travers N, Maldonado IL, Velut S. Child pial arteriovenous fistula of the conus medullaris presenting with spinal cord venous congestion: Case report and literature review. Interdiscip Neurosurg. 2021;25:101128.
Publication types
LinkOut - more resources
Full Text Sources