

Characterization of the Breast Cancer Liver Metastasis Microenvironment via Machine Learning Analysis of the Primary Tumor Microenvironment
- PMID: 39373616
- PMCID: PMC11525956
- DOI: 10.1158/2767-9764.CRC-24-0263
Characterization of the Breast Cancer Liver Metastasis Microenvironment via Machine Learning Analysis of the Primary Tumor Microenvironment
Abstract
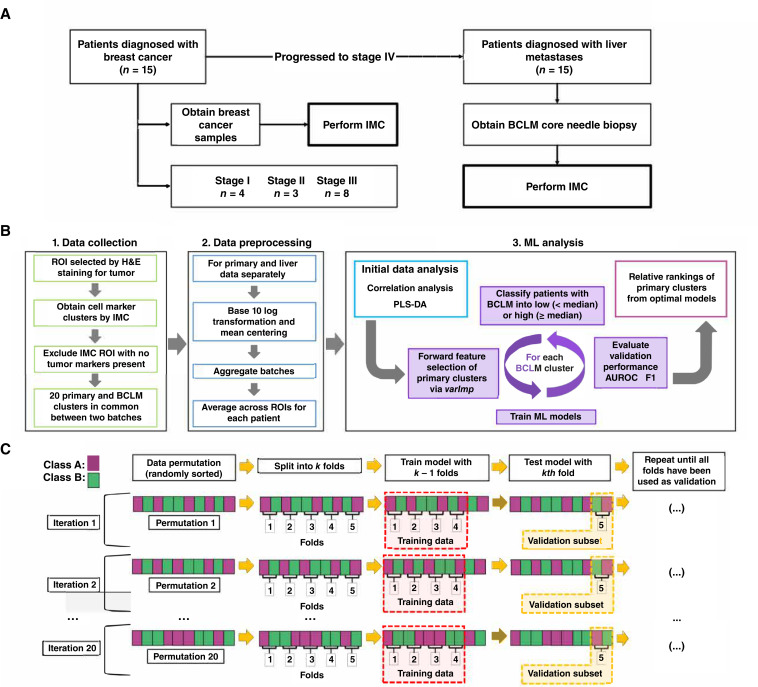
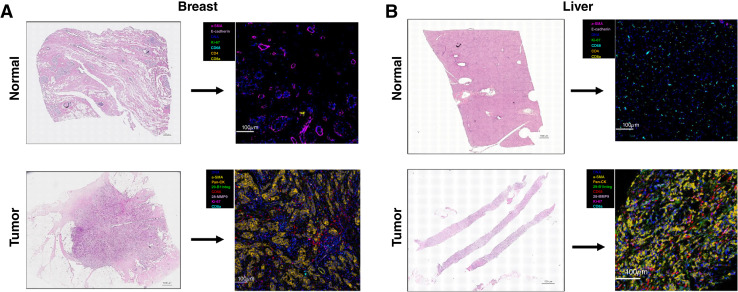
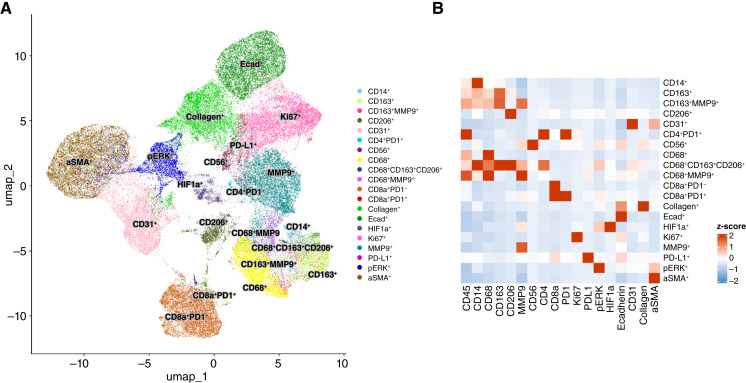
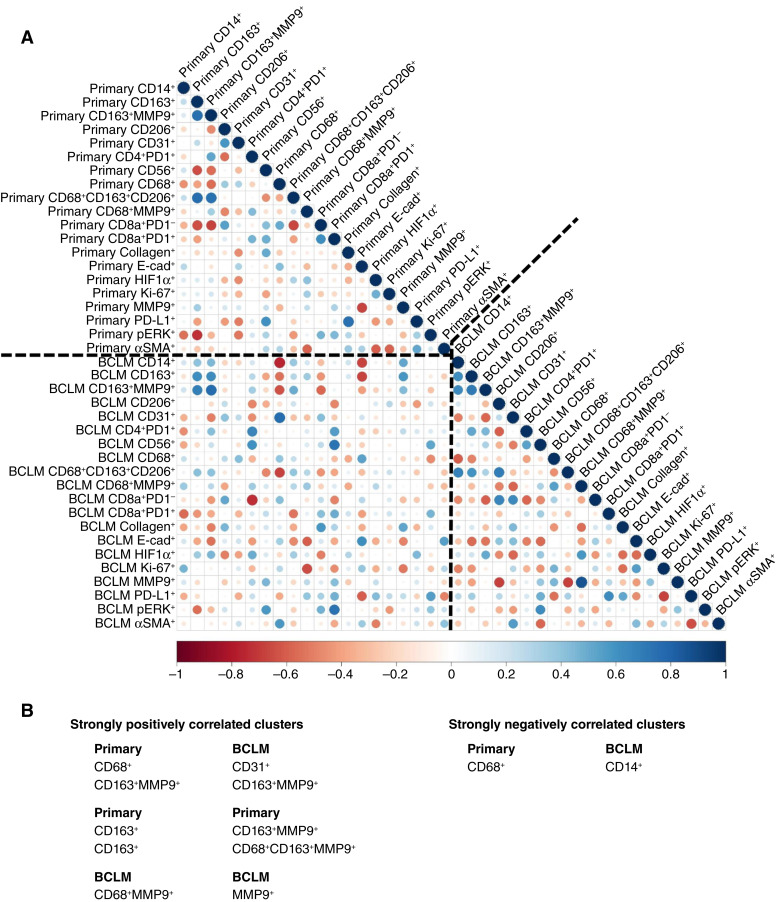
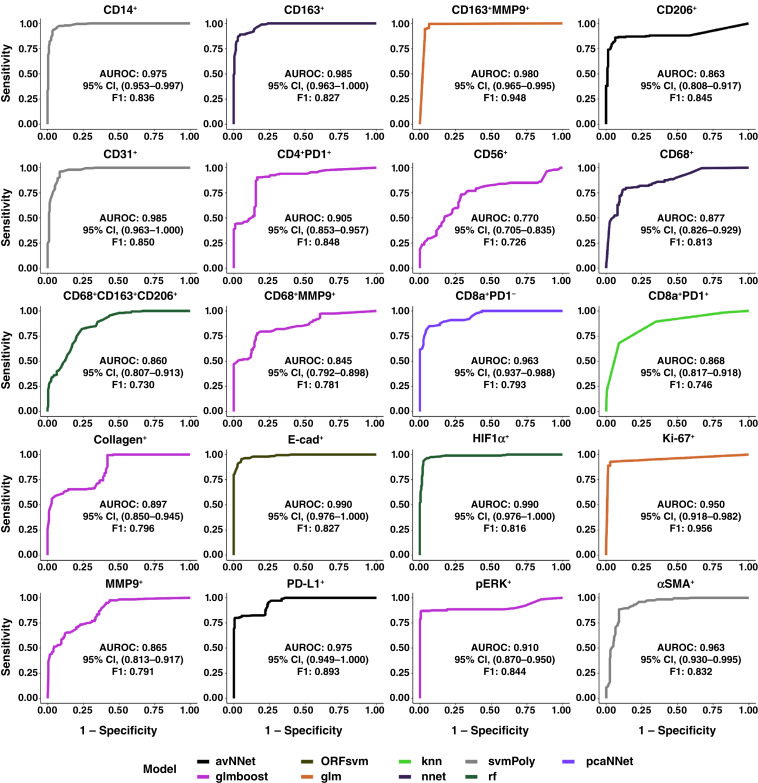
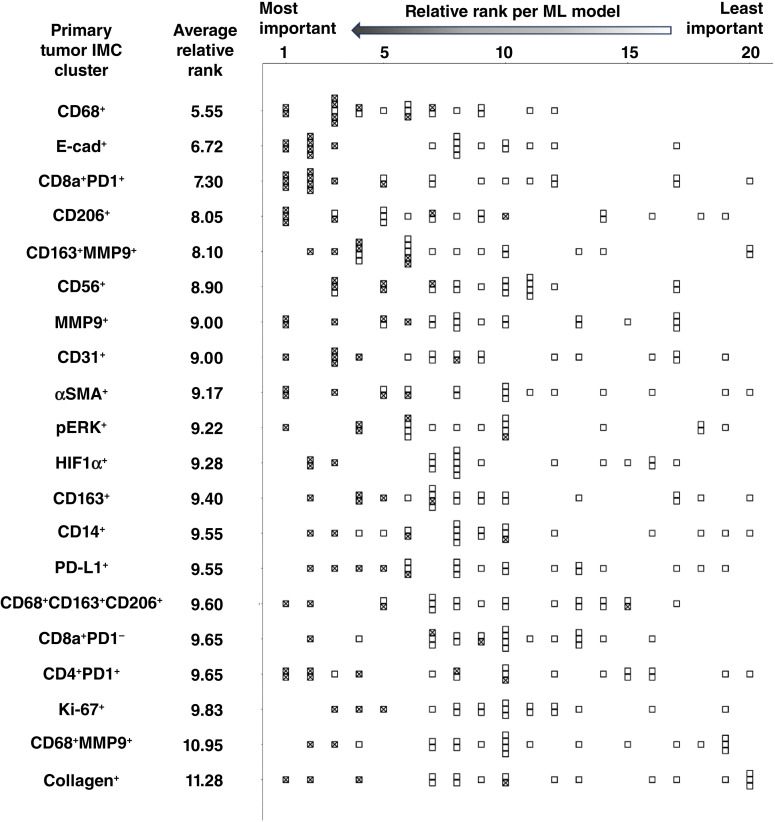
Breast cancer liver metastases (BCLM) are hypovascular lesions that resist intravenously administered therapies and have grim prognosis. Immunotherapeutic strategies targeting BCLM critically depend on the tumor microenvironment (TME), including tumor-associated macrophages. However, a priori characterization of the BCLM TME to optimize therapy is challenging because BCLM tissue is rarely collected. In contrast to primary breast tumors for which tissue is usually obtained and histologic analysis performed, biopsies or resections of BCLM are generally discouraged due to potential complications. This study tested the novel hypothesis that BCLM TME characteristics could be inferred from the primary tumor tissue. Matched primary and metastatic human breast cancer samples were analyzed by imaging mass cytometry, identifying 20 shared marker clusters denoting macrophages (CD68, CD163, and CD206), monocytes (CD14), immune response (CD56, CD4, and CD8a), programmed cell death protein 1, PD-L1, tumor tissue (Ki-67 and phosphorylated ERK), cell adhesion (E-cadherin), hypoxia (hypoxia-inducible factor-1α), vascularity (CD31), and extracellular matrix (alpha smooth muscle actin, collagen, and matrix metalloproteinase 9). A machine learning workflow was implemented and trained on primary tumor clusters to classify each metastatic cluster density as being either above or below median values. The proposed approach achieved robust classification of BCLM marker data from matched primary tumor samples (AUROC ≥ 0.75, 95% confidence interval ≥ 0.7, on the validation subsets). Top clusters for prediction included CD68+, E-cad+, CD8a+PD1+, CD206+, and CD163+MMP9+. We conclude that the proposed workflow using primary breast tumor marker data offers the potential to predict BCLM TME characteristics, with the longer term goal to inform personalized immunotherapeutic strategies targeting BCLM.
Significance: BCLM tissue characterization to optimize immunotherapy is difficult because biopsies or resections are rarely performed. This study shows that a machine learning approach offers the potential to infer BCLM characteristics from the primary tumor tissue.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
H.B. Frieboes and B. Godin report a grant from Department of Defense/US Army Medical Research during the conduct of the study. No disclosures were reported by the other authors.
Figures
References
-
- Sheafor DH, Frederick MG, Paulson EK, Keogan MT, DeLong DM, Nelson RC. Comparison of unenhanced, hepatic arterial-dominant, and portal venous-dominant phase helical CT for the detection of liver metastases in women with breast carcinoma. AJR Am J Roentgenol 1999;172:961–8. - PubMed
-
- Ginhoux F, Jung S. Monocytes and macrophages: developmental pathways and tissue homeostasis. Nat Rev Immunol 2014;14:392–404. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
