

Textbook outcome and nomogram-guided approaches for enhancing surgical success in elderly HCC patients: Deciphering the influence of sarcopenia
- PMID: 39373845
- PMCID: PMC11602817
- DOI: 10.1007/s13304-024-01992-3
Textbook outcome and nomogram-guided approaches for enhancing surgical success in elderly HCC patients: Deciphering the influence of sarcopenia
Abstract
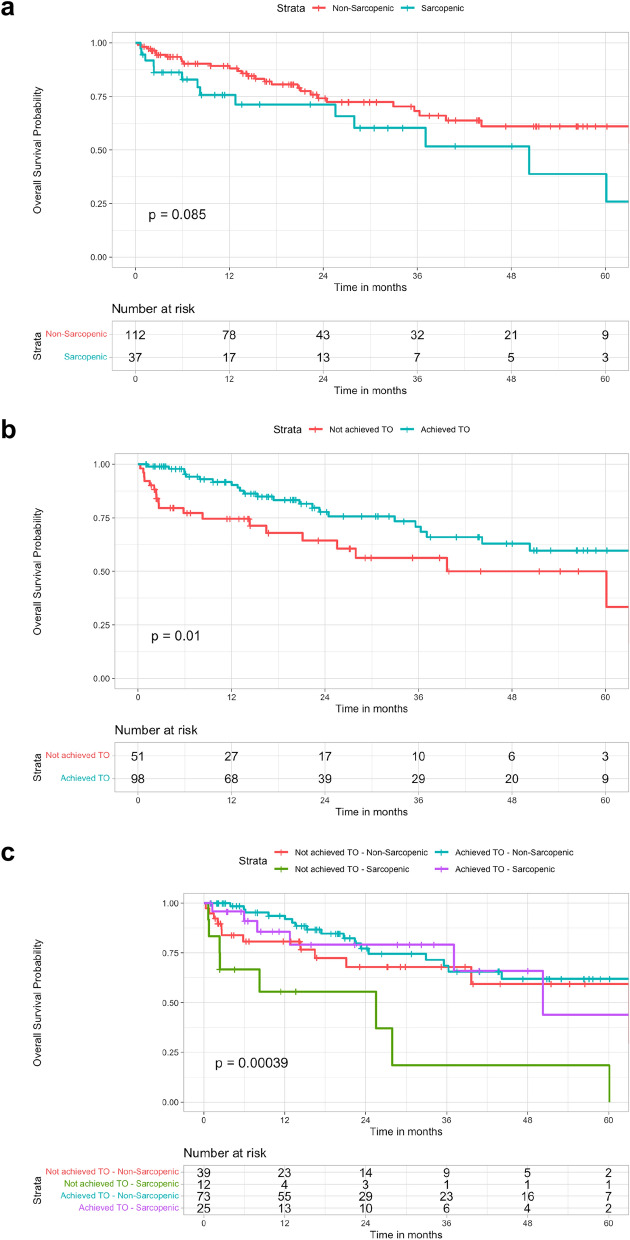
Sarcopenia, serving as a surrogate for frailty, is clinically significant in liver resection (LR) for elderly hepatocellular carcinoma (HCC) patients. Our study aims to assess sarcopenia's impact, measured by Psoas Muscle Index (PMI), on postoperative outcomes. We retrospectively studied patients aged ≥ 60 years who underwent LR for HCC between 2014 and 2018. PMI, derived from preoperative CT scans, and Textbook Outcome (TO) for LR were assessed. A nomogram predicting overall survival (OS) was developed via multivariable analysis. Of the 149 eligible HCC patients, the median PMI was 7.225 cm2/m2 in males and 4.882 cm2/m2 in females, with 37 (24.8%) patients identified as sarcopenic. Mortality was significantly associated with sarcopenia (HR 2.15; p = 0.032), MELD ≥ 10 (HR 3.13; p = 0.001), > 3 HCC nodules (HR 4.97; p = 0.001), and Clavien-Dindo ≥ 3 complications (HR 3.38; p < 0.001). Sarcopenic patients had a 5-year OS of 38.8% compared to 61% for non-sarcopenic individuals (p = 0.085). Achieving TO correlated with higher OS (p = 0.01). In sarcopenic cases, the absence of postoperative complications emerged as a limiting factor. Sarcopenic patients failing to achieve TO had worse OS compared to non-sarcopenic and TO-achieving counterparts (5-year OS 18.5%; p = 0.00039). Sarcopenia emerges as a prognostic factor for LR outcomes in elderly HCC patients. Postoperative complications in sarcopenic patients may compromise oncological outcomes.
Keywords: Cirrhosis; Hepatocellular carcinoma; Nomogram; Psoas muscle index; Sarcopenia; Textbook outcome.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no competing interests to declare that are relevant to the content of this article. Research involving human participants and/or animals: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This retrospective study involving human participants was conducted in accordance with the ethical standards of the institutional and national research committee and the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics board of Territorial Ethics Committee Central—Eastern Veneto Area (CET–ACEV)—Regional Resolution No. 330/2023 (protocol number 448n/A0/23, 18 January 2024). Informed consent: Each patient gave informed consent for every procedure performed and for the use of data for research and publication purposes.
Figures



References
-
- Petrowsky H, Clavien P-A (2005) Should we deny surgery for malignant hepato-pancreatico-biliary tumors to elderly patients? World J Surg 29:1093–1100 - PubMed
-
- Wang W, Zhu Y, Cheng J, Li M, Xia J, Hao J, Yu L, Lv Y, Wu Z, Wang B (2014) Major hepatectomy is safe for hepatocellular carcinoma in elderly patients with cirrhosis. Eur J Gastroenterol Hepatol 26:444–451 - PubMed
-
- Nozawa A, Kubo S, Takemura S, Sakata C, Urata Y, Nishioka T, Kinoshita M, Hamano G, Uenishi T, Suehiro S (2015) Hepatic resection for hepatocellular carcinoma in super-elderly patients aged 80 years and older in the first decade of the 21st century. Surg Today 45:851–857 - PubMed
-
- Cho SW, Steel J, Tsung A, Marsh JW, Geller DA, Gamblin TC (2011) Safety of liver resection in the elderly: how important is age? Ann Surg Oncol 18:1088–1095 - PubMed
-
- Allaire M, Gilgenkrantz H (2020) The aged liver: beyond cellular senescence. Clin Res Hepatol Gastroenterol 44:6–11 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
