

Severe bleeding events among critically ill patients with haematological malignancies
- PMID: 39373939
- PMCID: PMC11458868
- DOI: 10.1186/s13613-024-01383-2
Severe bleeding events among critically ill patients with haematological malignancies
Abstract
Background: Bleeding events are common complications in critically ill patients with haematological malignancies. The objective of this study was to assess the incidence and identify determinants of ICU-acquired severe bleeding events in critically ill patients with haematological malignancies. We conducted a single-center retrospective study including all adult patients with a history of haematological malignancy requiring unplanned ICU admission over a 12-year period (2007-2018). The primary endpoint was the occurrence of ICU-acquired (i.e. after the first 24 h in the ICU) severe bleeding events, as defined as grades 3 or 4 of the World Health Organization classification.
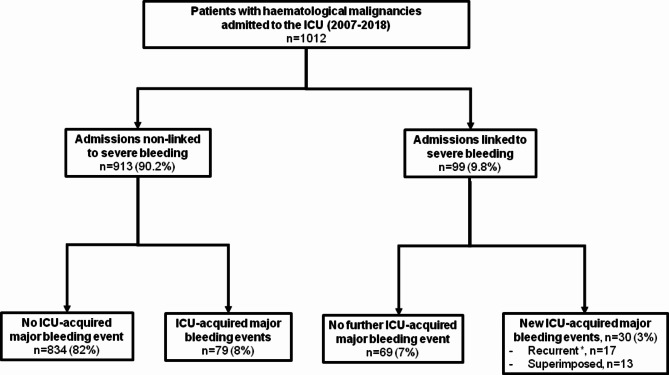
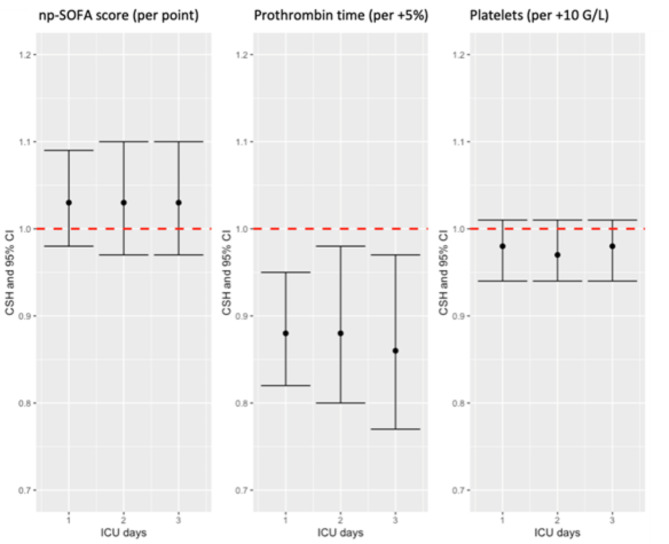
Results: A total of 1012 patients were analysed, mainly with a diagnosis of lymphoma (n = 434, 42.9%) and leukaemia or myelodysplastic syndrome (n = 266, 26.3%). Most patients were recently diagnosed (n = 340, 33.6%) and under active cancer treatment within the last 3 months (n = 604, 59.7%). The main cause for admission was infection (n = 479, 47.3%), but a significant proportion of patients were admitted for a primary haemorrhage (n = 99, 10%). ICU-acquired severe bleeding events occurred in 109 (10.8%) patients after 3.0 days [1.0-7.0] in the ICU. The main source of bleeding was the gastrointestinal tract (n = 44, 40.3%). Patients experiencing an ICU-acquired severe bleeding event displayed prolonged in-ICU length of stay (9.0 days [1.0-6.0] vs. 3.0 [3.5-15.0] in non-bleeding patients, p < 0.001) and worsened outcomes with increased in-ICU and in-hospital mortality rates (55% vs. 18.3% and 65.7% vs. 33.1%, respectively, p < 0.001). In multivariate analysis, independent predictors of ICU-acquired severe bleeding events were chronic kidney disease (cause-specific hazard 2.00 [1.19-3.31], p = 0.008), a primary bleeding event present at the time of ICU admission (CSH 4.17 [2.71-6.43], p < 0.001), non-platelet SOFA score (CSH per point increase 1.06 [1.01-1.11], p = 0.02) and prolonged prothrombin time (CSH per 5-percent increase 0.90 [0.85-0.96], p = 0.001) on the day prior to the event of interest.
Conclusions: Major bleeding events are common complications in critically ill patients with haematological malignancies and are associated with a worsened prognosis. We identified relevant risk factors of bleeding which may prompt closer monitoring or preventive measures.
Keywords: Critical care; Haematological malignancy; Haemorrhage; ICU-acquired bleeding; Thrombocytopenia.
© 2024. The Author(s).
Conflict of interest statement
FP: ALEXION PHARMA (institutional grant), GILEAD SCIENCES (consulting and teaching personal fees). MJ: ALEXION PHARMA (grant).
Figures
References
-
- Azoulay E, Mokart D, Pène F, Lambert J, Kouatchet A, Mayaux J, et al. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—A Groupe De Recherche Respiratoire en Réanimation Onco-Hématologique study. J Clin Oncol. 2013;31:2810–8. - DOI - PubMed
LinkOut - more resources
Full Text Sources
