

Cardiovascular Events After Chimeric Antigen Receptor T-Cell Therapy for Advanced Hematologic Malignant Neoplasms: A Meta-Analysis
- PMID: 39374017
- PMCID: PMC11459246
- DOI: 10.1001/jamanetworkopen.2024.37222
Cardiovascular Events After Chimeric Antigen Receptor T-Cell Therapy for Advanced Hematologic Malignant Neoplasms: A Meta-Analysis
Abstract
Importance: The frequency and clinical phenotypes of cardiotoxic events in chimeric antigen receptor (CAR) T-cell recipients remain poorly understood given that landmark approval trials typically exclude patients with high-risk cardiovascular profiles and data from nontrial settings are scarce.
Objective: To summarize the prevalence of adverse cardiovascular events among adults receiving CAR T-cell therapies for advanced hematologic malignant neoplasms.
Data sources: MEDLINE, Embase, Cochrane Library, and Google Scholar were systematically searched from database inception until February 26, 2024.
Study selection: Observational studies were included if they comprised adult CAR T-cell recipients with advanced hematologic malignant neoplasms and if they systematically evaluated cardiovascular complications.
Data extraction and synthesis: Extraction of prespecified parameters related to the patient population, study design, and clinical events was performed at the study level by 2 independent reviewers in accordance with the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) reporting guideline. Meta-analysis of single proportions was conducted using random-effect models with Freeman-Tukey double arcsine transformations to calculate pooled prevalence estimates. Sensitivity analysis was performed using generalized linear mixed models with logit transformations.
Main outcomes and measures: Ventricular and supraventricular arrhythmias, heart failure events, reduction in left ventricular ejection fraction, myocardial infarction, and cardiovascular and all-cause mortality.
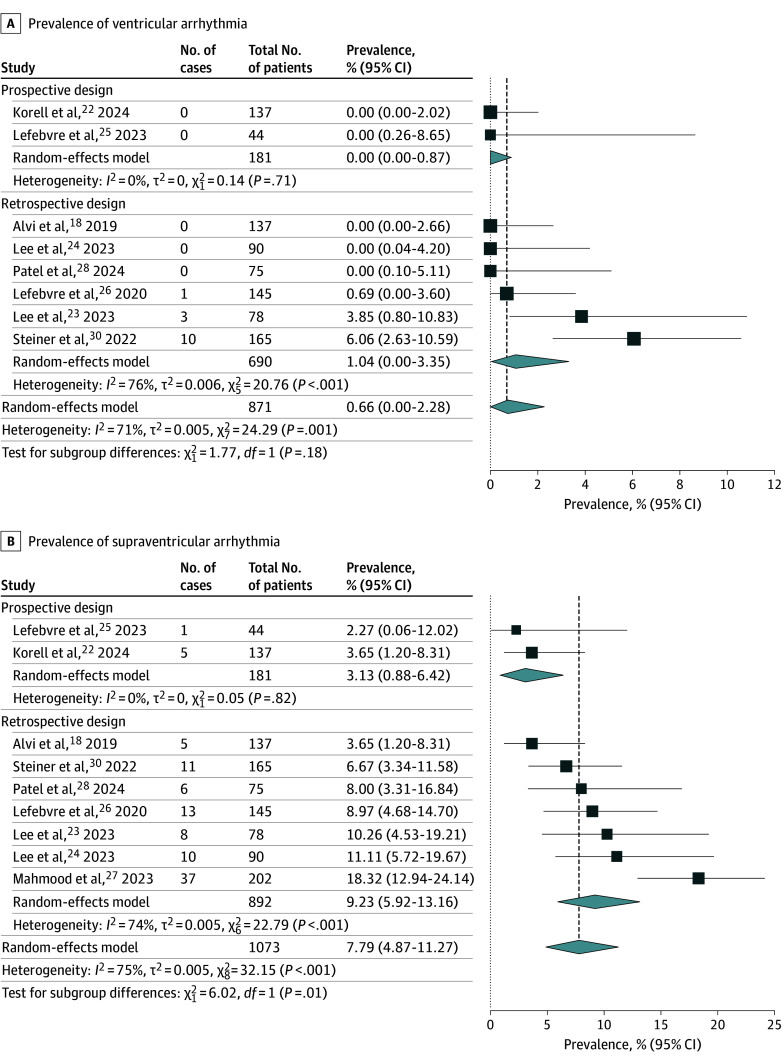
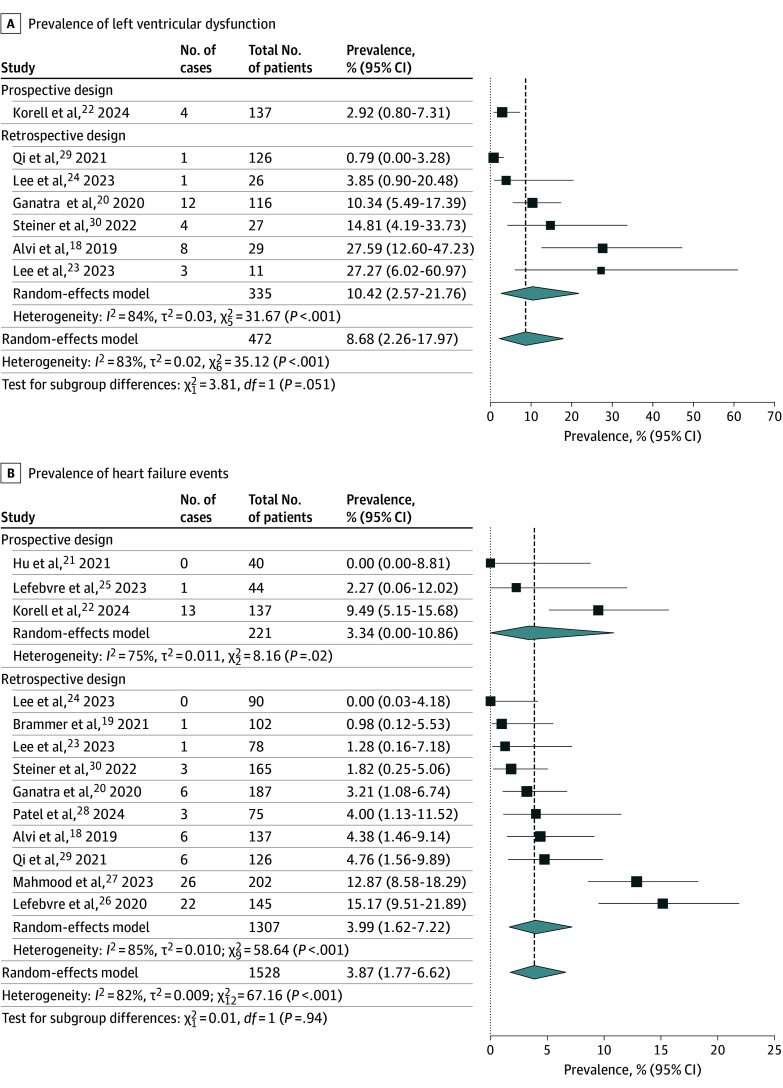
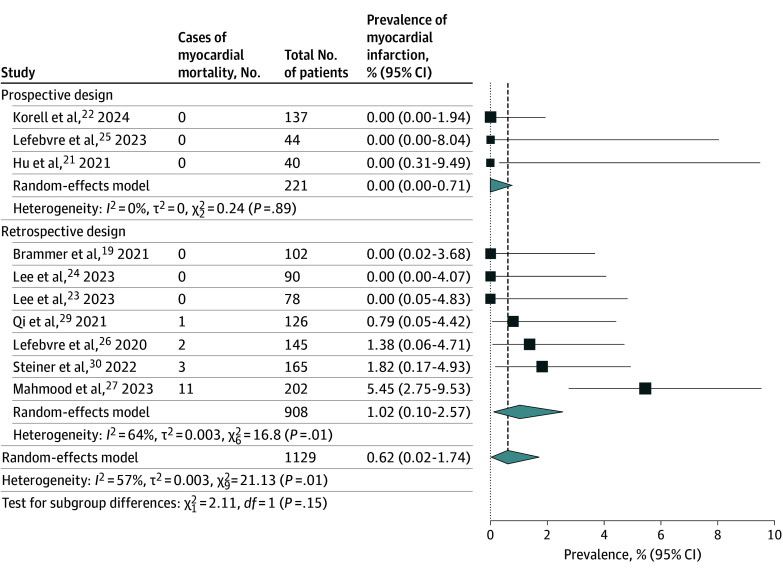
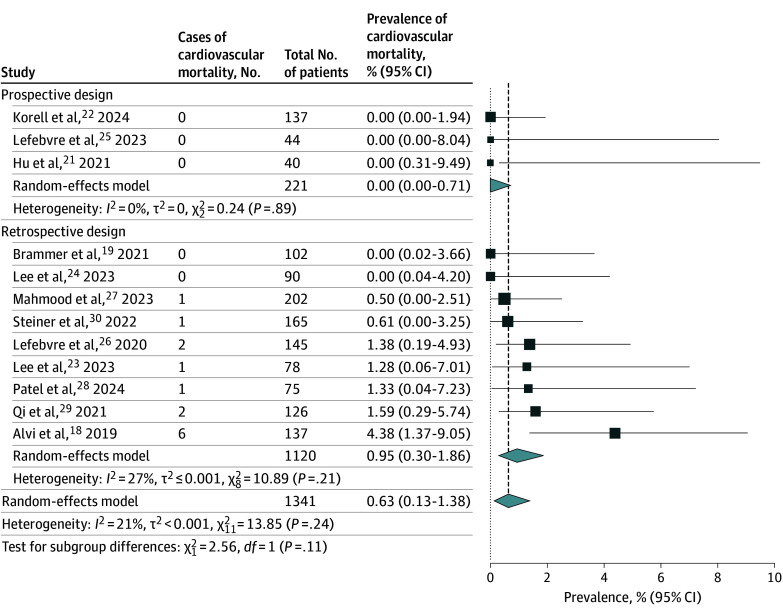
Results: Thirteen studies comprising 1528 CAR T-cell recipients (median [IQR] age, 61 [58.7-63.0] years; 1016 males [66%]; 80% patients with lymphoma) were included. The median (IQR) duration of follow-up was 487 (294-530) days. On random-effects meta-analysis, we observed a pooled prevalence of 0.66% (95% CI, 0.00%-2.28%) for ventricular arrhythmia, 7.79% (95% CI, 4.87%-11.27%) for supraventricular arrhythmia, 8.68% (95% CI, 2.26%-17.97%) for left ventricular dysfunction, 3.87% (95% CI, 1.77%-6.62%) for heart failure events, 0.62% (95% CI, 0.02%-1.74%) for myocardial infarction, and 0.63% (95% CI, 0.13%-1.38%) for cardiovascular death. The pooled prevalence of all-cause mortality was 30.01% (95% CI, 19.49%-41.68%). Sensitivity analyses generated similar findings.
Conclusions and relevance: This meta-analysis found a low prevalence of ventricular arrhythmia, myocardial infarction, and cardiovascular death among CAR T-cell recipients over a short-term to midterm follow-up. Left ventricular dysfunction and supraventricular arrhythmia were the most commonly reported cardiovascular complications, suggesting that cardiovascular surveillance strategies should focus on decreases in ejection fraction and supraventricular arrhythmia.
Conflict of interest statement
Figures
Comment in
-
Insights Into Cardiovascular Risks of Chimeric Antigen Receptor T-Cell Therapy-From Peril to Promise.JAMA Netw Open. 2024 Oct 1;7(10):e2437157. doi: 10.1001/jamanetworkopen.2024.37157. JAMA Netw Open. 2024. PMID: 39374023 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
